

Subscribe to RSS
DOI: 10.1055/s-0033-1364173
Angioleiomyoma of the Nasal Cavity
Authors
Address for correspondence
Publication History
18 July 2010
24 October 2010
Publication Date:
21 January 2014 (online)


Abstract
Introduction Vascular leiomyoma of the nasal cavity is an extremely rare tumor that represents less than 1% of all vascular leiomyomas. It is more prevalent in women between the fourth and sixth decades, reaching primarily the inferior nasal turbinates.
Objectives Reporting and assisting the systematization of more accurate diagnostic methods in clinical and complementary investigation of vascular leiomyoma in the nasal cavity.
Resumed Report We present the case of a 49-year-old woman diagnosed with vascular leiomyoma in the nasal cavity, which manifested mainly with nasal obstruction. During investigation, computer tomography was not diagnostic, the cytologic study was not conclusive, and according to the biopsy, it was a squamous papilloma.
Conclusion We suggest that the technical difficulty in obtaining an adequate amount of material for preoperative biopsy, associated with the topography of the lesion in the vestibular nasal region, may have contributed to changing the postoperative diagnosis. Thus, pathologic study of the surgical fragment is the more accurate method for diagnosis.
Keywords
clinical diagnosis - differential diagnosis - leiomyoma - inverted papilloma - nasal cavity - nasal obstruction - vascular leiomyoma - nasal cavity - squamous papilloma - diagnosisIntroduction
Angioleiomyoma or vascular leiomyoma is a rare benign tumor formed by smooth muscle cells in the vascular wall or by remnants of embryonic tissue, commonly found in the uterus (95%), skin (3%), and gastrointestinal tract (1.5%).[1] [2]
Less than 1% of all vascular leiomyomas occur in the nasal cavity.[3] [4] Hachisuga et al describe only 48 cases (8%) of angioleiomyoma in the head and neck in a study with 562 cases. Only 5 of the 48 cases were located in the nasal cavity, accounting for 1% of all angioleiomyomas.[5]
Maesaka et al reported the first case of angioleiomyoma in the nasal cavity in 1966.[6] Only 30 cases have been documented in English in the literature. Forty-nine additional cases have been reported in the Japanese literature.[7]
The origin of angioleiomyoma of the nasal cavity is uncertain, partly due to the scarcity of smooth muscle in the nasal cavity. Three hypotheses have been proposed for the origin of smooth muscle tumors in the nasal cavity: from aberrant undifferentiated mesenchymal cells; from elements of smooth muscle in the walls of blood vessels and of piloerector muscles; or from both previous hypotheses, simultaneously.[2] [8] [9] [10] [11] [12] [13] Some articles indicate that sexual hormones and Epstein-Barr virus infection can affect the genesis of nasal angioleiomyoma.[3] [12]
The literature shows a prevalence of angioleiomyomas of the nasal cavity in female patients (in a 2:1 ratio between females and males) between the fourth and sixth decades of life, and affecting mainly the inferior nasal conchae.[7] [9] These angioleiomyomas develop in the mucosa of the nasal cavity as single solid small cutaneous masses. They can be painful or not and can expand.[4] [12] They usually manifest as epistaxis (56.25%) and with nasal obstruction (56.25%).[11]
Computed tomography (CT) and magnetic resonance do not conclude the diagnosis. Cytologic examination does not provide a conclusive diagnosis. Surgical excision with histologic examination is the only way to make a definite diagnosis.[4] In addition to that, conventional light microscopy studies for the identification of angioleiomyoma after staining with hematoxylin-eosin can be performed using special staining, such as Masson trichrome stain, or immunohistochemical markers such as smooth muscle actin, desmin, myoglobin, S-100 protein, and vimentin. The absence of atypias is the most important histologic indication of benignity. The treatment of choice is total lesion excision.[2] [8] [10] [11] [12] [13] Recurrence is extremely rare after total excision.
In this report, we present the case of a 49-year-old woman with a diagnosis of angioleiomyoma of the nasal cavity.
Case Report
A 49-year-old woman was referred to the Department of Otolaryngology and Head and Neck Surgery of a tertiary hospital, in October 2008, with complaints of nasal obstruction and formation of scabs in the left nasal cavity for 12 years. In addition, pain and bulging in the external region of the nasal ipsilateral cavity were mentioned.
On physical examination and anterior rhinoscopy, a reddish mass was observed obstructing the whole left nasal cavity and vestibule, associated with a bulging in the left paranasal region. The oroscopy did not show anatomical morphologic changes.
Nasofibroscopy showed the presence of a reddish intracavitary sessile lesion in the inferior nasal concha, which occupied the whole left cavity and prevented the progression of the nasofibroscope. The cavum area was unobstructed.
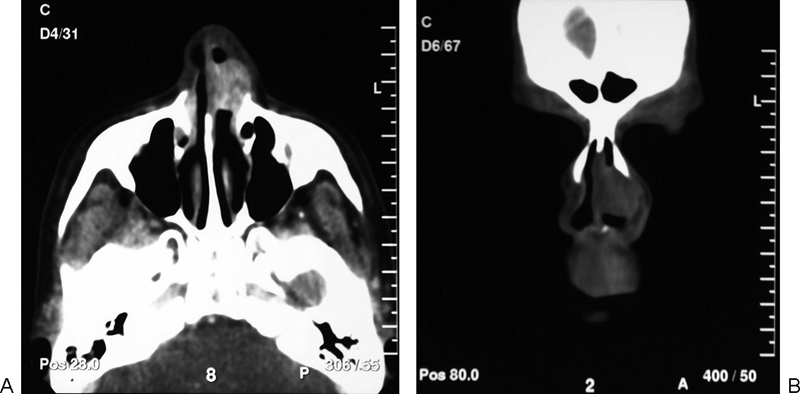
Given the clinical condition, a CT scan of the facial sinuses, biopsy of the lesion, and preoperative tests were ordered. The CT scan showed the presence of an oval lesion of soft tissue density that measured 2 cm in its longest axis, exhibited heterogeneous enhancement after injection of endovenous contrast, and was located in the left nasal cavity, in the transition between the cartilaginous and the bone parts of the nasal septum, in close contact with the latter ([Fig. 1]). The histopathologic examination showed a squamous papilloma with keratinization of the superficial mucosa without atypias, which confirmed the need to excise the lesion.
An incision was performed in the lateral mucosa of the left nasal cavity until the lesion was observed and pericapsular tissues were removed for total excision of the lesion. A nasal plug was inserted and a portion of the specimen was sent for anatomopathologic analysis.
The anatomopathologic result showed an irregular portion of brownish tissue of firm and elastic consistence measuring 1.6 × 1.5 × 1.1 cm. Microscopy revealed a benign lesion composed of multidirectional bundles of neoplastic smooth muscle cells with interspersed thick-walled vessels. The report stated angioleiomyoma as the diagnosis ([Fig. 2]).

Postoperatively, the surgical wound healed well with normal scarring. There was no report or signs of epistaxis. During the outpatient follow-up, the patient recovered asymptomatically and without relapse of the lesion.
Discussion
Leiomyomas of the nasal cavity are located in the nasal conchae, septum, paranasal sinuses, vestibule, and cavity floor.[12] Histologically, the vascular type is composed of bundles of relatively organized smooth muscle cells with interspersed thick-walled vessels. Vascular leiomyomas are less common.
The clinical diagnosis of vascular leiomyoma is complex. It is rarely included in the differential histopathologic diagnosis.[4] Other tumors of the nasal cavity are: nasal angiofibroma, hemangioma, inverted papilloma, malignant lymphoma, fibromyoma, leiomyoblastoma, hemangiopericytoma, angiosarcoma, angiomyolipoma, and vascular leiomyosarcoma.[10]
In the present case, the clinical diagnosis, which was based on anamnesis, physical examinations, and complementary tests, presented low sensitivity and reproducibility. During the assessment, a diagnosis of inverted papilloma was suggested, which required complementary tests for confirmation, according to the literature's scientific guidelines. The CT helped delineate and correlate the anatomical planes, surgical margins, and characterization of the intranasal mass; however, it did not provide specific conclusions. The preoperative biopsy did not coincide with the postoperative histologic study, because the total excision of the lesion (providing more and better-quality material) facilitates the anatomopathologic analysis. The surgical excision combined with the histologic study is the only way to make a definite diagnosis in these cases.[4] Depending on the extension and location of the lesion, its excision may be performed via endoscopy,[2] [8] [10] [11] [12] KTP532 laser,[2] or open surgery.[2] [3] [8] [12] Preoperative selective embolization should be considered for hypervascular or large lesions.
The patient did not have any relapse of the lesion during the 30 months of outpatient follow-up.
Conclusion
Angioleiomyoma of the nasal cavity is a rare benign tumor that is difficult to clinically diagnose and requires a detailed and invasive investigation. The complementary tests should guide the diagnostic reasoning; however, we concluded that it is essential to perform a postoperative anatomopathologic study to make a definite diagnosis of angioleiomyoma of the nasal cavity.
Acknowledgments
We thank Dr. Patrícia Maluf Cury, professor at the Department of Anatomical Pathology at the Hospital de Base de São José do Rio Preto for her essential collaboration in the preparation of slides, photos, and legends. We also thank the staff at SAME—Medical Archive Service—for their collaboration in providing medical records and radiological examinations. And we thank the reprography staff, who helped obtain the photo images from the radiologic examinations.
-
References
- 1 Enzinger FM, Lattes R, Torloni Internacional H. Classificação histológica de tumores: tipagem histológica dos tumores de tecidos moles. 2a ed. Geneva, Switzerland: Organização Mundial de Saúde—Springer Verlag; 1969
- 2 Marioni G, Marchese Ragona R, Fernandez S, Bruzon J, Staffieri M, Staffieri A. Expressão de receptores de progesterona em Angioleiomyoma da cavidade nasal. Acta Otolaryngol. 2002; 122: 408-412
- 3 Wang CP, Chang YL, Sheen TS. Vascular Leiomioma da cabeça e pescoço. Laryngoscope 2004; 114: 661-665
- 4 Chen CJ, Lai MT, Chen CY, Fang CL. Vascular leiomyoma of the nasal cavity: case report. Chin Med J (Engl) 2007; 120 (4) 350-352
- 5 Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma: a clinicopathologic reappraisal of 562 cases. Cancer 1984; 54: 126-130
- 6 Maesaka A, Keyaki Y, Nakahashi T. Nasal angioleiomyoma and leiomyosarcoma-report of 2 cases. Otologia (Fukuoka) 1966; 12: 42-47
- 7 Singh R, Hazarika P, Balakrishnan R, Gangwar N, Pujary P. Leiomyoma of the nasal septum. Indian J Cancer 2008; 45 (4) 173-175
- 8 Michael RC, Shah S. Angioleyomioma of the nasal cavity. Indian J Microbiol Pathol 2009; 52 (3) 386-388
- 9 Campelo VES, Neves M, Nakanishi MC, Voegels RL. Angioleiomioma de Cavidade nasal: relato de um caso e revisão de literatura. Braz J Otorhinolaryngol 2008; 74 (1) 147-150
- 10 Shankar PR, Subish P. Disease mongering. Singapore Med J 2007; 48 (4) 275-280
- 11 Ikeda K, Kuroda M, Sakaida N, Maehara M, Ohmura N, Sawada S. Cellular leiomyoma of the nasal cavity: findings of CT and MR imaging. AJNR Am J Neuroradiol 2005; 26: 1336-1338
- 12 Fonseca MT, Araújo PAK, Barreiros AC. Leiomioma de seio paranasal: Relato de um caso e revisão da literatura. Braz J Otorhinolaryngol 2002; 68 (3) 436-439
- 13 Cintra C. PPV, Lima WTA, AR Junior. Leiomioma da Cavidade nasal: relato de caso. Braz J Otorhinolaryngol 2007; 73 (6) 851
Address for correspondence
-
References
- 1 Enzinger FM, Lattes R, Torloni Internacional H. Classificação histológica de tumores: tipagem histológica dos tumores de tecidos moles. 2a ed. Geneva, Switzerland: Organização Mundial de Saúde—Springer Verlag; 1969
- 2 Marioni G, Marchese Ragona R, Fernandez S, Bruzon J, Staffieri M, Staffieri A. Expressão de receptores de progesterona em Angioleiomyoma da cavidade nasal. Acta Otolaryngol. 2002; 122: 408-412
- 3 Wang CP, Chang YL, Sheen TS. Vascular Leiomioma da cabeça e pescoço. Laryngoscope 2004; 114: 661-665
- 4 Chen CJ, Lai MT, Chen CY, Fang CL. Vascular leiomyoma of the nasal cavity: case report. Chin Med J (Engl) 2007; 120 (4) 350-352
- 5 Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma: a clinicopathologic reappraisal of 562 cases. Cancer 1984; 54: 126-130
- 6 Maesaka A, Keyaki Y, Nakahashi T. Nasal angioleiomyoma and leiomyosarcoma-report of 2 cases. Otologia (Fukuoka) 1966; 12: 42-47
- 7 Singh R, Hazarika P, Balakrishnan R, Gangwar N, Pujary P. Leiomyoma of the nasal septum. Indian J Cancer 2008; 45 (4) 173-175
- 8 Michael RC, Shah S. Angioleyomioma of the nasal cavity. Indian J Microbiol Pathol 2009; 52 (3) 386-388
- 9 Campelo VES, Neves M, Nakanishi MC, Voegels RL. Angioleiomioma de Cavidade nasal: relato de um caso e revisão de literatura. Braz J Otorhinolaryngol 2008; 74 (1) 147-150
- 10 Shankar PR, Subish P. Disease mongering. Singapore Med J 2007; 48 (4) 275-280
- 11 Ikeda K, Kuroda M, Sakaida N, Maehara M, Ohmura N, Sawada S. Cellular leiomyoma of the nasal cavity: findings of CT and MR imaging. AJNR Am J Neuroradiol 2005; 26: 1336-1338
- 12 Fonseca MT, Araújo PAK, Barreiros AC. Leiomioma de seio paranasal: Relato de um caso e revisão da literatura. Braz J Otorhinolaryngol 2002; 68 (3) 436-439
- 13 Cintra C. PPV, Lima WTA, AR Junior. Leiomioma da Cavidade nasal: relato de caso. Braz J Otorhinolaryngol 2007; 73 (6) 851