Subscribe to RSS
DOI: 10.1055/a-2750-5002
Medical Training on Climate Change and Health: Evaluation of an Online Learning Format for Outpatient Care
Article in several languages: English | deutschAuthors

Abstract
Background
Climate change increasingly affects public health and presents new challenges for outpatient care. Physicians require specific training opportunities to address these developments. As part of the project AdaptNet (“Adapting primary and specialised outpatient care to the health impacts of climate change”), an online training course on climate change and health was developed to provide essential foundational knowledge on climate-related health risks and adaptation strategies for medical practice. The aim of this study was to evaluate the training in terms of comprehensibility, applicability, and its relevance to medical practice.
Methods
The training was provided as an online learning format. The evaluation followed a mixed-methods approach involving 23 general practitioners and specialised physicians from the Northern Bavaria region (Germany). Data collection included a standardised online questionnaire as well as structured group discussions. The analysis was guided by the Consolidated Framework for Implementation Research, with data being evaluated using qualitative content analysis and quantitative descriptive methods.
Results
The quantitative analysis showed that the training was perceived as comprehensible, practically relevant, and well-structured. Participants considered the scope and duration of the training to be appropriate. The multimedia design was particularly positively highlighted. The qualitative results indicated increased awareness of climate-related health risks and a high perceived added value for medical practice. The training generated great interest among participants and was considered relevant for outpatient care. The flexible integration of the online format into daily work routines was seen as advantageous. Critical feedback referred to the lack of opportunities for interactive exchange and a desire for additional regional adaptation of the training content.
Conclusion
Climate change and adaptation are recognised as relevant topics in medical practice and can be effectively and practically communicated in the outpatient sector through the online training developed specially for this purpose. Regional customisation of the training content appears sensible in order to address climate and health challenges more specifically. Online formats may prove to be suitable tools for effective knowledge transfer.
Keywords
Klimawandel - Anpassungsmaßnahmen - ambulante Versorgung - Online-Schulung - Evaluation - WeiterbildungBackground
Climate change represents one of the major health challenges of the 21st century. Outpatient medical care is increasingly confronted with heat-related illnesses, respiratory conditions, and vector-borne infections, all of which are associated with the rising frequency of extreme weather events and environmental changes [1]. In response to these developments, the World Health Organisation (WHO) has called for measures to strengthen the resilience of health systems. This recommendation is echoed in national policy frameworks such as the German Strategy for Adaptation to Climate Change, adopted in 2008, and the Federal Climate Change Adaptation Act, which came into effect in 2024 [2] [3]. Despite these policy frameworks, the German healthcare system remains inadequately prepared for the health impacts of climate change, particularly with respect to the care of vulnerable populations, including older adults, people with chronic illnesses, and those experiencing social disadvantage [4] [5] [6]. Early and preventive interventions at the level of primary and specialist outpatient care are essential to mitigate climate-related health risks and prevent avoidable hospital admissions [7]. However, these efforts require healthcare professionals to possess a sound understanding of climate-related health effects and practical adaptation strategies. Current studies indicate that physicians in outpatient care often lack access to suitable training programmes, evidence-based guidelines, and practice-oriented tools to support climate adaptation [8] [9] [10]. To enhance the climate resilience of outpatient care, urgent action is needed in the areas of medical education and continuing professional development.
As part of the project AdaptNet (“Adapting primary and specialised outpatient care to the health impacts of climate change”), a practice-oriented toolbox for climate change adaptation is being developed for outpatient care [11] [12]. The tools are designed to support both general practitioners and specialists in outpatient care in implementing preventive adaptation measures, as well as in the early identification and management of health impacts related to climate change. The tools are intended to enable low-threshold integration of climate-related health aspects into everyday practice and thus contribute to strengthening climate resilience in the outpatient sector. A central element of the toolbox is an online training programme for physicians on climate change and health. This article describes the evaluation of the developed training programme in terms of its comprehensibility, applicability and content relevance.
Method
Development and didactic concept of the online training course
The development of the training programme “Climate Change and Health” [13] followed a participatory and iterative approach based on the methodology of Intervention Mapping [14]. It was informed by a comprehensive literature review and a quantitative needs assessment (online questionnaire) conducted between April and May 2023. In this assessment, physicians (n=67) from general practitioner and specialist outpatient practices were surveyed regarding the requirements for climate-adapted healthcare delivery and necessary adaptation measures in the outpatient sector [15]. The findings provided relevant insights and needs, which served, among other things, as a foundation for the initial drafts and the selection of training materials by the Heidelberg University Hospital (AH, JN, CQ). To ensure a practice-oriented and target-group-appropriate design, these drafts were revised and further developed based on feedback from general practitioners and specialist physicians (e. g., internal medicine, cardiology, endocrinology, surgery, and psychosomatic medicine) affiliated with the healthcare network “Quality and Efficiency” (QuE) in Nuremberg (Germany) [16]. The developed training aims to highlight the relevance of climate change for outpatient medical care and to convey concrete, practical adaptation strategies for medical practices. Its didactic structure is guided by the taxonomy of cognitive learning objectives developed by Bloom et al. (1956) [17], combining knowledge transfer with practical, application-oriented content. The training is based on the “Climate Change and Health” curriculum issued by the German Medical Association (2022) [18] as well as existing, field-tested materials, including the format “Climate Change – What Changes for Patient Care?” [19] developed by the Heidelberg University Hospital (AH, CQ, JN), and analyses conducted by the Chair of Regional Climate Change and Health at the University of Augsburg (IKO, FA, EH) [4] [20] [21].
Further development involved academic and partly clinically active experts from relevant disciplines, who contributed short video lectures and literature recommendations. The content was systematically prepared, supplemented with quiz questions and reflection tasks, and professionally validated. The training programme follows a self-directed, flexible learning format tailored to the needs of practising physicians. Reflection tasks supported the transfer into practice by encouraging participants to critically examine existing routines and integrate new content into their daily work. The training was made freely available as an online course on the HIGH-edu.courses platform, a Massive Open Online Course (MOOC) initiative by the Heidelberg Institute of Global Health [22]. It is modular in structure, designed to take approximately 90 minutes to complete, and consists of three thematic modules, each comprising several units.
Module 1 – Overview and basics:
-
Planetary Health, Climate Change and Health: Introduction to the concept of Planetary Health and the key links between climate change and health.
-
Health effects of climate change: overview of key health consequences and adaptation strategies in the healthcare system; supplemented by results from the AdaptNet project on doctors' perceptions.
-
Regional climate risks for health: Presentation of specific regional health risks due to climate change (e. g., heat stress, pollen count).
Module 2 – Medical specialisations:
-
Heat: Relevant health risks due to heat and practical adaptation strategies for outpatient care.
-
Allergies: Link between climate change and allergy incidence.
-
Infectious diseases: Thematic block on climate-related changes in infection risks.
-
Mental health: climate change-related stress and mental illness.
Module 3 – Additional Resources and Information:
-
Summary of key content and reflection
-
The AdaptNet toolbox for climate change adaptation
-
Climate action in medical practices
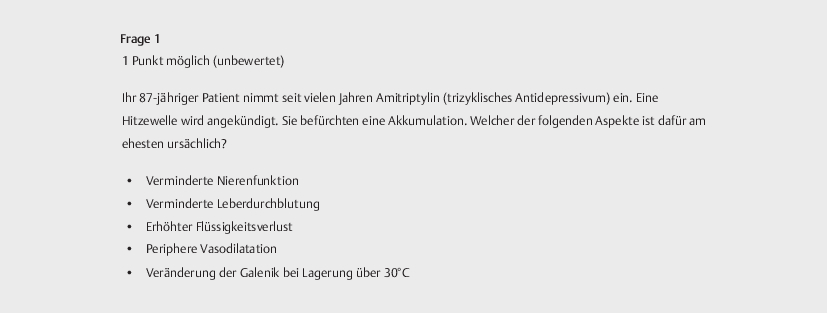
Each chapter consists of an introductory section, a core knowledge component, and optional in-depth modules. A variety of materials are used to convey the content, including videos, specialist texts, scientific articles, and visual summaries (e. g., tables, figures). At the end of each chapter, quiz questions allow for individual knowledge assessment ( [Fig. 1] ).

Evaluation of the online training
The development and implementation of the toolbox was accompanied by a formative process evaluation conducted by the University Hospital Erlangen (StSt, SH, MK). This evaluation was guided by the framework proposed by Hulscher et al. [23] and the recommendations of the Medical Research Council [24]. The aim was to enable continuous revision and context-specific adaptation of the tools based on the active involvement and feedback of the physicians involved. A central element of this process evaluation was the evaluation of the online training, which was carried out between April and September 2023. A total of 23 general practitioners and specialist physicians from the QuE Nuremberg healthcare network took part in the training and tested it. The participants were recruited via existing contacts from QuE and through direct outreach, including their newsletters and informational events by the network. They received financial compensation for their participation as well as continuing medical education (CME) points. The evaluation was carried out using a mixed-methods approach in two phases: (1) immediately after completion of the training using a standardised online questionnaire (Online-Appendix 1), (2) in September 2023 as part of structured observations of a medical quality circle for joint reflection on the content.
The analysis was based on the theoretical framework of the Consolidated Framework for Implementation Research (CFIR) [25], which recognises success factors and obstacles in the implementation of health instruments along several dimensions. The insights gained were directly incorporated into the ongoing development of the training content and methodology, complementing the formative evaluation with specific information on practical feasibility in medical settings:
-
Intervention characteristics refer to features of the instrument itself, such as the content, and were applied to assess the innovation and substance of the training during evaluation (e. g., training content and its novelty).
-
Inner setting describes the internal structures that influence implementation and was applied in the evaluation to the structure, format and practicability of the training (e. g., design, practical applicability).
-
Outer setting refers to external factors, such as specifications and needs, and was applied to the need and transferability of the training (e. g., need for the training, possibility of transferring it to other contexts and target groups).
-
Characteristics of individuals include the characteristics of the people involved, such as their motivation, added value and the acceptability of the instrument, which were also transferred in our evaluation (e. g., perceived benefit for the participants).
Online questionnaire
The online questionnaire was developed by the University Hospital Erlangen (StSt, SH, MK) and administered using REDCap (Research Electronic Data Capture) [26]. The software was used to programme the questionnaire and for anonymous data collection and administration [27]. At the beginning of the questionnaire, the participants were informed about the voluntary nature of their participation, the data protection concept and the storage of the anonymously collected data. The questionnaire was created based on the content of the online training along the dimensions of the CFIR and tested for comprehensibility within the project team. In the pre-test, ambiguities were discussed and items adapted using the thinking-aloud method [28]. The questionnaire contains a total of 33 questions, which are divided into five sections:
-
Evaluation of the content and format of the training course using a five-point Likert scale (1=strongly disagree, 5=strongly agree)
-
Evaluation of the media using a five-point Likert scale (1=not at all helpful, 5=very helpful)
-
Closed questions on the duration and scope of the training
-
Open questions regarding further suggestions
-
Demographic data (gender, years of professional experience, type of practice).
The name of the physician was not collected for reasons of data protection and to avoid potential inferences.
Group discussion
At the end of the pilot phase, the training was reflected on and discussed with the physicians based on the format of a 60-minute world café [29 ] (Online-Appendix 2). The structured observation [30] was conducted using an observation guide developed by the University Hospital Erlangen (StSt, SH, MK) (Online-Appendix 3). The guideline was tested for comprehensibility within the project team using the thinking-aloud method [28]. The 23 participants were divided into four small groups of five to six persons, with each group focusing on a different dimension of the CFIR:
-
Group 1 “Innovation and content” (intervention characteristics): Content of the training that the participants particularly remember and what prior knowledge they already had.
-
Group 2 “Needs and transferability” (Outer setting): Training needs and acceptance in terms of time and financial aspects.
-
Group 3 “Structure, format and feasibility” (inner setting): Format of the training, its media design, and the availability of training materials.
-
Group 4 “Acceptance and added value” (Characteristics of individuals): Motivation of participants, perceived relevance and potential benefits of the training.
Each table was moderated by one or two members of the project team (AH, JN, CQ, StSt, MK, SH), who documented the discussion manually using the observation guide. Efforts were made to record key statements as close to verbatim as possible. The group discussions were not audio-recorded in order to maintain a natural discussion atmosphere and to minimise potential bias arising from participants' increased awareness of being recorded. The small group discussions lasted 45 minutes, after which the results were summarised in a plenary session and final feedback was obtained from the participating physicians.
Analysis and report
The quantitative data was analysed using descriptive statistics with IBM SPSS V.27 and is reported as mean values (M) and the standard deviations (SD). The answers in the open text field were categorised and summarised. The qualitative data was analysed using qualitative content analysis based on Mayring [31]. The data sets from both surveys were analysed and interpreted along the dimensions of the CFIR. The results are presented in accordance with the guidelines for reporting the results of internet-based surveys (CHERRIES) [32] and the consolidated criteria for reporting qualitative research (COREQ) [33].
Results
Sample
The sample ([Table 1]) comprised 23 participants. Their professional experience ranged between 20 and 41 years. Around two thirds (63.6%) were female and the majority of participants (60.9%) worked in a joint practice. Most physicians were based in general practice or internal medicine (80%).
|
Variable |
Category |
n |
|---|---|---|
|
Participants |
Total |
23 |
|
Mean (M) |
29.86 |
|
|
Professional experience (years) |
Min |
20.00 |
|
Max |
41.00 |
|
|
Standard deviation (SD) |
6.359 |
|
|
Gender |
Female |
15 (63.6%) |
|
Male |
8 (36.4%) |
|
|
Type of practice |
Joint |
14 (60.9%) |
|
Single |
9 (391%) |
Quantitative results
Innovation and content
Almost two thirds (65.2%) of the physicians had previously taken part in a medical training course on climate change. On average, the participants agreed that the content of the training was clearly defined (M=4.17, SD=0.491) and that the connection between climate change and health was explained in an understandable way (M=4.52, SD=0.511). The participants stated that they learnt a lot of new things about the topic (M=3.74, SD=0.915) and that the training helped them to better understand the concept of planetary health (M=4.22, SD=0.422) ([Table 2]).
|
Domain |
Item |
M |
SD |
|---|---|---|---|
|
Innovation and content |
Content of the training was clearly defined. |
4.17 |
0.49 |
|
Connection between climate change and health was understandable. |
4.52 |
0.51 |
|
|
I learnt a lot of new things. |
3.74 |
0.92 |
|
|
Better understanding of planetary health. |
4.22 |
0.42 |
|
|
Structure, format and feasibility |
Online format was appropriate. |
4.26 |
0.54 |
|
Structure and format were comprehensible. |
4.30 |
0.64 |
|
|
Selected media were appropriate. |
4.26 |
0.54 |
|
|
Videos were best rated. |
4.39 |
0.50 |
|
|
Need and transferability |
Learning objectives were met. |
4.17 |
0.49 |
|
Relevance for outpatient care made clear. |
4.04 |
0.37 |
|
|
Could apply what was learnt in practice. |
4.30 |
0.64 |
|
|
Content useful for practical application. |
4.17 |
0.58 |
|
|
Acceptance and added value |
Would recommend the training to others. |
4.17 |
0.58 |
|
Learnt something useful for medical practice. |
4.09 |
0.42 |
|
|
Training was too demanding (rejected). |
1.91 |
1.04 |
|
|
No added value for practice (rejected). |
1.91 |
1.00 |
Structure, format and feasibility
The implementation of the training in an online format was rated as appropriate (M=4.26, SD=0.541). Almost three quarters of respondents found the structure and format to be comprehensible (M=4.30, SD=0.635). The selected media (videos, graphics, components) were rated also as appropriate (M=4.26, SD=0.541). The videos were rated the best (M=4.39, SD=0.499) ([Table 2]).
The scope of the training was predominantly perceived positively, with 82.6% stating that the scope was just right and 17.4% denying this. The latter stated that the training was too extensive. The in-depth materials/modules were viewed by 69.6%, who also found them informative, and 56.5% found them also helpful. The majority (78.3%) felt that the duration of the 90-minute training course was just right, while 21.7% rated it as too long.
Need and transferability
The training met expectations in terms of learning objectives (M=4.17, SD=0.491) and familiarised participants with the relevance of climate change for outpatient care (M=4.04, SD=0.367). The majority could imagine applying what they had learnt in their practice (M=4.30, SD=0.635). The training content was perceived as useful for practical application (M=4.17, SD=0.576) ([Table 2]).
Acceptance and added value
Almost all would recommend the training to others (M=4.17, SD=0.576) and stated that they had learnt something useful for their medical practice (M=4.09, SD=0.417). The statements that the training was too demanding (M=1.91, SD=1.041) or offered no added value for the practice (M=1.91, SD=0.996) were rejected ([Table 2]).
Open text field
With regard to the innovation and content of the training course, the multimedia presentation and the variety of topics were particularly emphasised. In terms of structure, format and practicability, there was both positive feedback and suggestions for improvement. Suggestions for further dissemination of the training and the need for additional thematic content were mentioned in relation to need and transferability. The dimension of acceptance and added value was not addressed in the open text field ([Table 3]).
|
Dimension |
Feedback |
Response |
n |
|---|---|---|---|
|
Innovation and Content |
Positive |
Media: Videos, quiz, multimedia presentation; materials well prepared |
7 |
|
Information: Detailed insights from various medical disciplines |
4 |
||
|
Strong topics: Adaptation options for older people; lecture on medication; current debates and facts |
3 |
||
|
Structure, Format and Feasibility |
Positive |
Training style: Lively, varied, concise |
3 |
|
Online format: Ability to take breaks; can be integrated into daily routine |
2 |
||
|
Negative |
Media: More videos; tables in videos partly too small, text illegible when enlarged |
2 |
|
|
Structure: A brief summary and conclusion would be helpful |
2 |
||
|
Organisation: Simpler structuring of chapters |
1 |
||
|
Suggestion |
Quiz questions: Difficult to interpret; unnecessarily challenging; distracting; no solutions provided |
3 |
|
|
Media: Short video clips on heat-related behaviour for waiting room screens available for download |
2 |
||
|
Materials: Practical tools and politicisation: More urgent roll-out to all, not only vulnerable groups; more practical tools for doctors; encouragement of political engagement and duty to inform |
2 |
||
|
Needs and Transferability |
Suggestion |
Practical tools and politicisation: More urgent roll-out to all, not only vulnerable groups; more practical tools for doctors; encouragement of political engagement and duty to inform |
2 |
|
Additional topics: How doctors can positively influence climate change; more on different medications and sustainability |
2 |
||
|
Acceptance and Added Value |
– |
– |
– |
Qualitative results
Innovation and content
The participating physicians reported that the online training promoted a common understanding of climate change and planetary health, so that all participants had a common basis for the discussion. They were particularly impressed by the dynamics of climate change and its far-reaching consequences for the healthcare system. This emphasised the need for adaptation measures: “Adaptations in care, treatment and practice are urgently needed!” (I04). The participants intensively discussed the adaptation of medication, which they considered to be increasingly important in view of rising temperatures. Another key topic was the spread of vectors and the increased occurrence of new diseases that are favoured by changing climatic conditions. In particular, the spread of new vectors such as ticks or the Asian tiger mosquito and the associated health risks were discussed as key challenges. The participants stated that they had gained new insights into the spread of vector-borne diseases.
The physicians particularly emphasised the fact that the training conveyed specific adaptation measures in a practical way: “There was a lot of new content that was well presented, especially the specific adaptation measures” (I20). Although the participants recognised the value of the training in providing basic knowledge, they also saw challenges in the practical implementation of the adaptation measures. Many praised the fact that the training also included the topic of sustainability: “Where can we become more sustainable in practice? I also think this is an important topic!” (I08). The training also raised awareness of the increasing challenges posed by climate change in the healthcare sector, including the “increase in exsiccosis and hospital admissions caused by heat” (I21). The training drew attention to existing initiatives and several participants were pleasantly surprised by the number of them. In this context, the participants also emphasised the AdaptNet project, which they considered to be timely and particularly relevant in view of the necessary adaptation measures for outpatient care.
Structure, format and feasibility
The majority responded very positively to the online format and favoured it because it could be flexibly integrated into their everyday working life: “Online was easy to implement alongside everyday practice, you could set your own pace” (I05). The physicians found a face-to-face event too time-consuming, particularly because of the travelling involved. They appreciated the fact that the online format allowed them to take breaks, as the training took longer than initially expected. Several rated the effort-benefit factor of the training as positive and also found the platform used to be user-friendly: “The training was well structured and didactically well implemented” (I03). The fact that participants were able to access the content at any time to read up on it was emphasised as positive, while individual criticism was voiced of the quiz questions, some were perceived as too difficult and had offered no resolution. With regard to the use of media, the mixture of visual and audio content was praised, and the videos in particular were considered to be great. Some were motivated and completed the in-depth material in full, while others found the effort involved too high and therefore used it less: “The ambition to complete all the material to the end was there, but the effort was too high” (I12). The possibility of downloading the training materials was seen as a great advantage. Many participants printed out the documents and also wanted a compact manual (e. g., PDF) or handout for practical use.
Need and transferability
Many physicians rated the need for training on climate change and health as high and at the same time emphasised that this should be regionally oriented, for example with regard to specific topics such as heat or medication adaptation and tailored to the respective target group. The participants emphasised the relevance of such training not only for physicians, but also for medical assistants, patients and other healthcare professions (e. g., nurses and pharmacists). According to the participants, the training content should be integrated into the training programmes for medical students and postgraduate medical trainees. Educational institutions such as schools were also named as useful target groups for raising awareness of climate change and its health consequences at an early stage. The physicians suggested that such training should be made mandatory by state health authorities: “The offer and obligation of such training should come from the health authorities” (I18). The participants clearly showed that neither an expense allowance nor CME points were necessary to ensure their participation in the training. Instead, they expressed a desire to make the training course accessible to all target groups free of charge. Their participation was predominantly based on intrinsic motivation.
Acceptance and added value
The training raised participants' awareness of the urgency and danger of the issue, as one person reported: “It got me involved, but also scared me about how dangerous climate change is” (I02). In addition to a noticeable emotional involvement, the participants also perceived the training as informative and practically relevant. Several people emphasised that the training did not provide an opportunity to exchange ideas with colleagues. An interactive component within the training platform was desired in order to ask questions and to network with each other: “It would have been great to be able to ask questions or exchange ideas again afterwards” (I09). The physicians rated the training as highly relevant for providing information and passing on knowledge. A positive effect was that the training strengthened their confidence in argumentation when talking to patients and helped them to consolidate and deepen their own knowledge in a targeted manner. In their opinion, sound knowledge is essential in order to be able to properly inform and educate not only patients, but also colleagues and the practice team: “It's important to be able to provide information, you need sound knowledge for this” (I15). The Participants reported that the training encouraged them to engage with the topic of climate change, increased their awareness of it and also led to further reflection in everyday practice, in the practice team and in their private lives. During the discussion, the physicians repeatedly referred to the perceived environmental changes and the increasing health burdens: “Climate change has an impact on humanity, we really have to do something” (I22).
Discussion
The evaluation results illustrate the high level of importance attributed to climate change and adaptation in medical practice and outpatient care, and they are consistent with international findings that call for a rapid strengthening of the resilience and adaptive capacity of health systems [34]. Participants rated the perceived need for training as very high. Accordingly, they expressed support for more firmly embedding climate and adaptation topics within medical education and continuing professional development. An extension to other healthcare professions and educational institutions was also recommended. A concern that the WHO highlights as a key element of climate-resilient and low-emission health systems [35]. The integration of relevant content into undergraduate and postgraduate training was regarded as essential for ensuring sustainable outpatient care under the conditions of climate change [36]. In Germany, the integration of planetary health learning objectives into the “NKLM/ÄApprO” provides a concrete framework for embedding the corresponding competencies into curricula [37]. For outpatient care, recent studies demonstrate increased awareness and clear expectations regarding adaptation measures, while also revealing gaps in knowledge, routine, and responsibilities, underscoring the need for targeted training and implementation programmes [9].
The participating physicians regarded the topic climate adaptation as highly relevant to outpatient care and viewed the training as a key tool for addressing this need. The content was perceived as practical, accessible, and well-structured. Participants particularly highlighted that the training contributed to raising awareness of climate-related health risks and offered concrete approaches for implementing preventative measures. International studies likewise show that targeted training can increase the awareness of climate risks in health care and strengthen the capacity to act [38]. The comprehensibility and structure of the training were rated positively. The ease with which the online format could be integrated into everyday clinical practice was seen as a significant benefit. Further studies indicate that digital formats, particularly in the context of climate change, offer the advantage of being able to update content rapidly and adapt flexibly to new developments [39] [40].
The Participants also advocated for adapting the training to regional circumstances in the event of broader implementation, in order to prepare outpatient practices more specifically for the local impacts of climate change. In the literature, this finding is supported by evidence that climatic stresses vary regionally and therefore require differentiated content [20]. Institutional analyses, such as the German Environment Agency’s report on heat action plans, likewise underscore the relevance of regionally adapted measures. Accordingly, recent studies emphasise that tailoring training content in a differentiated manner can make an essential contribution to addressing local health challenges in a targeted way [41] [42].
Strengths and limitations
Strengths of the study include the structured evaluation based on the CFIR and the mixed-methods approach, which enabled a nuanced analysis. Particular emphasis should be placed on the active involvement of physicians, who had contributed to the development and testing of the training and provided specific feedback. Despite the small sample size (n=23), the qualitative data offer a valuable complement to the quantitative findings. Further research with larger and more heterogeneous samples is recommended to assess the effectiveness and transferability of the training.
One limitation is that only physicians from a regional healthcare network were included, within which the topics of climate and health had already been discussed. This may have introduced bias due to heightened climate awareness among the participants. As the group discussions were not audio-recorded and key statements could only be documented manually, subjective bias cannot be ruled out. Additionally, social desirability bias may have influenced responses, as participants received remuneration and CME points. A further limitation is that the evaluation focused solely on perceived relevance and applicability from the participants’ perspective, an evidence-based assessment of effectiveness was not conducted and remains the subject of future research.
Conclusion
This work demonstrates that climate change and adaptation are recognised as relevant topics in medical practice as well as outpatient care and can be communicated effectively and practice-oriented through online trainings. The training developed represents a suitable format for promoting knowledge of climate-related health risks and adaptation strategies within the ambulatory sector. Successful implementation requires clear, flexible content, consideration of regional specificities, and early involvement of the target group(s). Integrating such training into continuing medical education programmes may make an important contribution to strengthening climate resilience in the healthcare system.
Ethics
The study was approved by the Ethics Committees of the Medical Faculty of Heidelberg University (S-163/2023) and Friedrich-Alexander University Erlangen-Nürnberg (23-296-S/2023).
Data Availability
Anonymised data (quantitative and qualitative) are available upon justified request to the principal investigators and solely for research purposes. The principal investigators will review any analysis proposal and assess its consistency with the scientific objectives of the AdaptNet project.
Additional Data and Information
Additional data (Appendix 1: RedCAP questionnaire, Appendix 2: World Café (discussion points), Appendix 3: observation guide) associated with this article can be found in the online version. Access to the online course “Climate Change and Health” is available via the following link: https://high-edu.courses/courses/course-v1:HIGH+AdaptNet1+2024.2/course/
Declaration on the Use of Generative AI in Scientific Writing
During the writing process of this paper, the authors used ChatGPT as a tool for grammatical phrasing of individual sentences. After using this tool, the authors reviewed and edited the content and take full responsibility for the final version of the publication.
Funding Information
Innovationsfond des gemeinsamen Bundesausschusses — 01VSF22044
Conflict of Interest
Alina Herrmann and Claudia Quitmann have received honoraria for the design of training sessions on climate change–related topics within the framework of general practitioner training programs. Both are members of the Deutsche Allianz Klimawandel und Gesundheit e.V. (KLUG); this membership is not associated with any financial compensation. Alina Herrmann is the spokesperson for the Climate Change and Health section of the German Society for General Practice and Family Medicine (DEGAM); this position is also unpaid. All other authors declare no conflicts of interest.
Acknowledgements
We would like to sincerely thank the physicians of the Gesundheitsnetz Qualität und Effizienz Nürnberg for their dedicated participation in the AdaptNet project.
-
References
- 1 Watts N, Amann M, Arnell N. et al. The 2019 report of The<em>Lancet</em>Countdown on health and climate change: ensuring that the health of a child born today is not defined by a changing climate. The Lancet 2019; 394: 1836-1878
- 2 (WHO) WHO. Operational framework for building climate resilient health systems.
2015 [Available from https://www.who.int/publications/i/item/9789240081888]
- 3 BMUV. Die Deutsche Anpassungsstrategie an den Klimawandel 2025 [Available
from: https://www.bmuv.de/themen/klimaanpassung/die-deutsche-anpassungsstrategie-an-den-klimawandel?utm_source=chatgpt.com]
- 4 Hertig E, Hunger I, Kaspar-Ott I. et al. Klimawandel und Public Health in Deutschland – Eine Einführung in den Sachstandsbericht Klimawandel und Gesundheit 2023. Journal of Health Monitoring. 2023 (S3)
- 5 Winklmayr C, Matthies-Wiesler F, Muthers S. et al. Hitze in Deutschland: Gesundheitliche Risiken und Maßnahmen zur Prävention. Journal of Health Monitoring. 2023: 3-34
- 6 Augustin J, Burkart K, Endlicher W. et al. Klimawandel und Gesundheit. Springer; 2023
- 7 Ansah EW, Amoadu M, Obeng P. et al. Health systems response to climate change adaptation: a scoping review of global evidence. BMC Public Health 2024; 24: 2015
- 8 Mezger NCS, Thöne M, Wellstein I. et al. Climate protection in practices – current status, motivation and challenges in outpatient care. Z Evid Fortbild Qual Gesundhwes 2021; 166: 44-54
- 9 Litke NA, Poß-Doering R, Fehrer V. et al. Building climate resilience: awareness of climate change adaptation in German outpatient medical practices. BMC Health Services Research 2024; 24: 184
- 10 Armand W, Padget M, Pinsky E. et al. Clinician Knowledge and Attitudes About Climate Change and Health After a Quality Incentive Program. JAMA Netw Open 2024; 7: e2426790
- 11 (G-BA) GBI. AdaptNet – Adaptation und Vernetzung der haus- und fachärztlichen
Versorgung im Hinblick auf die gesundheitlichen Auswirkungen des Klimawandels
2023 [Available from: https://innovationsfonds.g-ba.de/projekte/versorgungsforschung/adaptnet.554]
- 12 Nürnberg GQ. AdaptNet- Werkzeugkoffer: Klima-Toolbox für die Arztpraxis 2025
[Available from: https://www.gesundheitsnetznuernberg.de/adaptnet-klima-toolbox/]
- 13 High-edu.courses H. Ärztliche Basisschulung Klimawandel und Gesundheit 2025
- 14 Bartholomew LK, Parcel GS, Kok G. Intervention mapping: a process for developing theory- and evidence-based health education programs. Health Educ Behav 1998; 25: 545-563
- 15 Nieder J, Quitmann C, Hueber S. et al. What makes physicians implement climate change and heat adaptation measures in outpatient practices?. A mixed-methods study Climate-resilient Health Systems, Elsevier Public Health. 2025
- 16 Gesundheitsnetz QuE Nürnberg 2025 [Available from: https://www.gesundheitsnetznuernberg.de/]
- 17 Bloom BS, Engelhart MD, Furst EJ. et al. Taxonomy of educational objectives: The classification of educational goals. Handbook I: Cognitive domain. 1956
- 18 Bundesärztekammer. Curriculum Klimawandel und Gesundheit. 2022; 1. Aufl.,
Fassung vom 23.09.2022
- 19 High-edu.courses H. Klimawandel – Was ändert sich für die Patientenversorgung?
2024 [Available from: https://high-edu.courses/courses/course-v1:HIGH+CCdoc.2+2022.T1/about]
- 20 Alvarez F, Kaspar-Ott I, Herrman A. et al. Estimation of Health Risks from Climate Change-Related Hazards Using the Example of Nuremberg, Germany. SSRN. 2025
- 21 Hertig E. Health-relevant ground-level ozone and temperature events under future climate change using the example of Bavaria, Southern Germany. Air Quality, Atmosphere & Health 2020; 13: 435-446
- 22 High-edu.courses H. MOOCs (Massive Open Online Courses) 2025 [Available
from: https://high-edu.courses/tos]
- 23 Hulscher ME, Laurant MG, Grol RP. Process evaluation on quality improvement interventions. Qual Saf Health Care 2003; 12: 40-46
- 24 Moore GF, Audrey S, Barker M. et al. Process evaluation of complex interventions: Medical Research Council guidance. Bmj 2015; 350: h1258
- 25 Damschroder LJ, Reardon CM, Widerquist MAO. et al. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci 2022; 17: 75
- 26 Erlangen U. REDCap Produktivsystem des Universitätsklinikums Erlangen. 2025 [Available from: https://redcap.uk-erlangen.de/]
- 27 Harris PA, Taylor R, Thielke R. et al. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics 2009; 42: 377-381
- 28 Konrad K. Lautes Denken. In: Mey G, Mruck K, editors. Handbuch Qualitative Forschung in der Psychologie. Wiesbaden: Springer Fachmedien Wiesbaden; 2019: 1-21
- 29 Brown J, Isaacs D. The World Café: Shaping Our Futures Through Conversations That Matter. Berrett-Koehler Publishers; 2005
- 30 Kauffeld S. Strukturierte Beobachtung. In: Kühl S, Strodtholz P, Taffertshofer A, editors. Handbuch Methoden der Organisationsforschung: Quantitative und Qualitative Methoden. Wiesbaden: VS Verlag für Sozialwissenschaften;; 2009: 580-599
- 31 Mayring P, Fenzl T. Qualitative Inhaltsanalyse. In: Baur N, Blasius J, editors. Handbuch Methoden der empirischen Sozialforschung. Wiesbaden: Springer Fachmedien Wiesbaden; 2019: 633-648
- 32 Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res 2004; 6: e34
- 33 Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007; 19: 349-357
- 34 Romanello M, Walawender M, Hsu S-C. et al. The 2024 report of the<em>Lancet</em>Countdown on health and climate change: facing record-breaking threats from delayed action. The Lancet 2024; 404: 1847-1896
- 35 (WHO) WHO. Operational framework for building climate resilient and low carbon health systems. 2023
- 36 Rybol L, Nieder J, Amelung D. et al. Integrating climate change and health topics into the medical curriculum – a quantitative needs assessment of medical students at Heidelberg University in Germany. GMS J Med Educ 2023; 40: Doc36
- 37 Wabnitz K, Schwienhorst-Stich EM, Asbeck F. et al. National Planetary Health learning objectives for Germany: A steppingstone for medical education to promote transformative change. Front Public Health 2022; 10: 1093720
- 38 Hathaway J, Maibach EW. Health Implications of Climate Change: a Review of the Literature About the Perception of the Public and Health Professionals. Current Environmental Health Reports 2018; 5: 197-204
- 39 Dockweiler C, Stark AL, Albrecht J. editors. Settingbezogene Gesundheitsförderung und Prävention in der digitalen Transformation: Transdisziplinäre Perspektiven. 2023. Baden-Baden: Nomos Verlagsgesellschaft mbH & Co. KG.;
- 40 Sorensen C, Campbell H, Depoux A. et al. Core competencies to prepare health professionals to respond to the climate crisis. PLOS Clim 2023; 2: e0000230
- 41 Debora J, Kaiser T, Christian K. et al. Analyse von Hitzeaktionsplänen und gesundheitlichen Anpassungsmaßnahmen an Hitzeextreme in Deutschland. Umwelt & Gesundheit. 2023 03/2023
- 42 Perreault-Carranza T, Ni V, Savoie J. et al. Core Competencies of the Public Health Workforce in Climate Change and Extreme Weather Events Preparedness, Response, and Recovery: A Scoping Review. International Journal of Environmental Research and Public Health 2024; 21: 1233
Correspondence
Publication History
Received: 25 June 2025
Accepted after revision: 20 October 2025
Accepted Manuscript online:
18 November 2025
Article published online:
23 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Watts N, Amann M, Arnell N. et al. The 2019 report of The<em>Lancet</em>Countdown on health and climate change: ensuring that the health of a child born today is not defined by a changing climate. The Lancet 2019; 394: 1836-1878
- 2 (WHO) WHO. Operational framework for building climate resilient health systems.
2015 [Available from https://www.who.int/publications/i/item/9789240081888]
- 3 BMUV. Die Deutsche Anpassungsstrategie an den Klimawandel 2025 [Available
from: https://www.bmuv.de/themen/klimaanpassung/die-deutsche-anpassungsstrategie-an-den-klimawandel?utm_source=chatgpt.com]
- 4 Hertig E, Hunger I, Kaspar-Ott I. et al. Klimawandel und Public Health in Deutschland – Eine Einführung in den Sachstandsbericht Klimawandel und Gesundheit 2023. Journal of Health Monitoring. 2023 (S3)
- 5 Winklmayr C, Matthies-Wiesler F, Muthers S. et al. Hitze in Deutschland: Gesundheitliche Risiken und Maßnahmen zur Prävention. Journal of Health Monitoring. 2023: 3-34
- 6 Augustin J, Burkart K, Endlicher W. et al. Klimawandel und Gesundheit. Springer; 2023
- 7 Ansah EW, Amoadu M, Obeng P. et al. Health systems response to climate change adaptation: a scoping review of global evidence. BMC Public Health 2024; 24: 2015
- 8 Mezger NCS, Thöne M, Wellstein I. et al. Climate protection in practices – current status, motivation and challenges in outpatient care. Z Evid Fortbild Qual Gesundhwes 2021; 166: 44-54
- 9 Litke NA, Poß-Doering R, Fehrer V. et al. Building climate resilience: awareness of climate change adaptation in German outpatient medical practices. BMC Health Services Research 2024; 24: 184
- 10 Armand W, Padget M, Pinsky E. et al. Clinician Knowledge and Attitudes About Climate Change and Health After a Quality Incentive Program. JAMA Netw Open 2024; 7: e2426790
- 11 (G-BA) GBI. AdaptNet – Adaptation und Vernetzung der haus- und fachärztlichen
Versorgung im Hinblick auf die gesundheitlichen Auswirkungen des Klimawandels
2023 [Available from: https://innovationsfonds.g-ba.de/projekte/versorgungsforschung/adaptnet.554]
- 12 Nürnberg GQ. AdaptNet- Werkzeugkoffer: Klima-Toolbox für die Arztpraxis 2025
[Available from: https://www.gesundheitsnetznuernberg.de/adaptnet-klima-toolbox/]
- 13 High-edu.courses H. Ärztliche Basisschulung Klimawandel und Gesundheit 2025
- 14 Bartholomew LK, Parcel GS, Kok G. Intervention mapping: a process for developing theory- and evidence-based health education programs. Health Educ Behav 1998; 25: 545-563
- 15 Nieder J, Quitmann C, Hueber S. et al. What makes physicians implement climate change and heat adaptation measures in outpatient practices?. A mixed-methods study Climate-resilient Health Systems, Elsevier Public Health. 2025
- 16 Gesundheitsnetz QuE Nürnberg 2025 [Available from: https://www.gesundheitsnetznuernberg.de/]
- 17 Bloom BS, Engelhart MD, Furst EJ. et al. Taxonomy of educational objectives: The classification of educational goals. Handbook I: Cognitive domain. 1956
- 18 Bundesärztekammer. Curriculum Klimawandel und Gesundheit. 2022; 1. Aufl.,
Fassung vom 23.09.2022
- 19 High-edu.courses H. Klimawandel – Was ändert sich für die Patientenversorgung?
2024 [Available from: https://high-edu.courses/courses/course-v1:HIGH+CCdoc.2+2022.T1/about]
- 20 Alvarez F, Kaspar-Ott I, Herrman A. et al. Estimation of Health Risks from Climate Change-Related Hazards Using the Example of Nuremberg, Germany. SSRN. 2025
- 21 Hertig E. Health-relevant ground-level ozone and temperature events under future climate change using the example of Bavaria, Southern Germany. Air Quality, Atmosphere & Health 2020; 13: 435-446
- 22 High-edu.courses H. MOOCs (Massive Open Online Courses) 2025 [Available
from: https://high-edu.courses/tos]
- 23 Hulscher ME, Laurant MG, Grol RP. Process evaluation on quality improvement interventions. Qual Saf Health Care 2003; 12: 40-46
- 24 Moore GF, Audrey S, Barker M. et al. Process evaluation of complex interventions: Medical Research Council guidance. Bmj 2015; 350: h1258
- 25 Damschroder LJ, Reardon CM, Widerquist MAO. et al. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci 2022; 17: 75
- 26 Erlangen U. REDCap Produktivsystem des Universitätsklinikums Erlangen. 2025 [Available from: https://redcap.uk-erlangen.de/]
- 27 Harris PA, Taylor R, Thielke R. et al. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics 2009; 42: 377-381
- 28 Konrad K. Lautes Denken. In: Mey G, Mruck K, editors. Handbuch Qualitative Forschung in der Psychologie. Wiesbaden: Springer Fachmedien Wiesbaden; 2019: 1-21
- 29 Brown J, Isaacs D. The World Café: Shaping Our Futures Through Conversations That Matter. Berrett-Koehler Publishers; 2005
- 30 Kauffeld S. Strukturierte Beobachtung. In: Kühl S, Strodtholz P, Taffertshofer A, editors. Handbuch Methoden der Organisationsforschung: Quantitative und Qualitative Methoden. Wiesbaden: VS Verlag für Sozialwissenschaften;; 2009: 580-599
- 31 Mayring P, Fenzl T. Qualitative Inhaltsanalyse. In: Baur N, Blasius J, editors. Handbuch Methoden der empirischen Sozialforschung. Wiesbaden: Springer Fachmedien Wiesbaden; 2019: 633-648
- 32 Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res 2004; 6: e34
- 33 Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007; 19: 349-357
- 34 Romanello M, Walawender M, Hsu S-C. et al. The 2024 report of the<em>Lancet</em>Countdown on health and climate change: facing record-breaking threats from delayed action. The Lancet 2024; 404: 1847-1896
- 35 (WHO) WHO. Operational framework for building climate resilient and low carbon health systems. 2023
- 36 Rybol L, Nieder J, Amelung D. et al. Integrating climate change and health topics into the medical curriculum – a quantitative needs assessment of medical students at Heidelberg University in Germany. GMS J Med Educ 2023; 40: Doc36
- 37 Wabnitz K, Schwienhorst-Stich EM, Asbeck F. et al. National Planetary Health learning objectives for Germany: A steppingstone for medical education to promote transformative change. Front Public Health 2022; 10: 1093720
- 38 Hathaway J, Maibach EW. Health Implications of Climate Change: a Review of the Literature About the Perception of the Public and Health Professionals. Current Environmental Health Reports 2018; 5: 197-204
- 39 Dockweiler C, Stark AL, Albrecht J. editors. Settingbezogene Gesundheitsförderung und Prävention in der digitalen Transformation: Transdisziplinäre Perspektiven. 2023. Baden-Baden: Nomos Verlagsgesellschaft mbH & Co. KG.;
- 40 Sorensen C, Campbell H, Depoux A. et al. Core competencies to prepare health professionals to respond to the climate crisis. PLOS Clim 2023; 2: e0000230
- 41 Debora J, Kaiser T, Christian K. et al. Analyse von Hitzeaktionsplänen und gesundheitlichen Anpassungsmaßnahmen an Hitzeextreme in Deutschland. Umwelt & Gesundheit. 2023 03/2023
- 42 Perreault-Carranza T, Ni V, Savoie J. et al. Core Competencies of the Public Health Workforce in Climate Change and Extreme Weather Events Preparedness, Response, and Recovery: A Scoping Review. International Journal of Environmental Research and Public Health 2024; 21: 1233