

Subscribe to RSS
DOI: 10.1055/a-2738-7298
Peroral cholangioscopy-guided laser lithotripsy using a thin cholangioscope under balloon enteroscopy for Roux-en-Y anastomosis
Authors

Although balloon enteroscopy is helpful, stone extraction in patients with Roux-en-Y anastomosis can be very difficult, particularly in cases with multiple large stones [1] [2]. Recently, a thin cholangioscope (eyeMAX; Micro-Tech, China) with a length of 219 cm and a diameter of 9-Fr ([Fig. 1]) has enabled peroral cholangioscopy (POCS)-guided interventions to be performed under balloon enteroscopy [3]. POCS-guided intraductal interventions using either laser lithotripsy or electrohydraulic lithotripsy (EHL) can facilitate the extraction of difficult stones [4] [5]. It has been reported that, compared with EHL, laser lithotripsy provides the advantage of more precise stone targeting, thereby reducing the risk of injury to the surrounding tissue [3]. We report a case of successful laser lithotripsy using a thin cholangioscope under balloon enteroscopy in a patient with Roux-en-Y anastomosis.

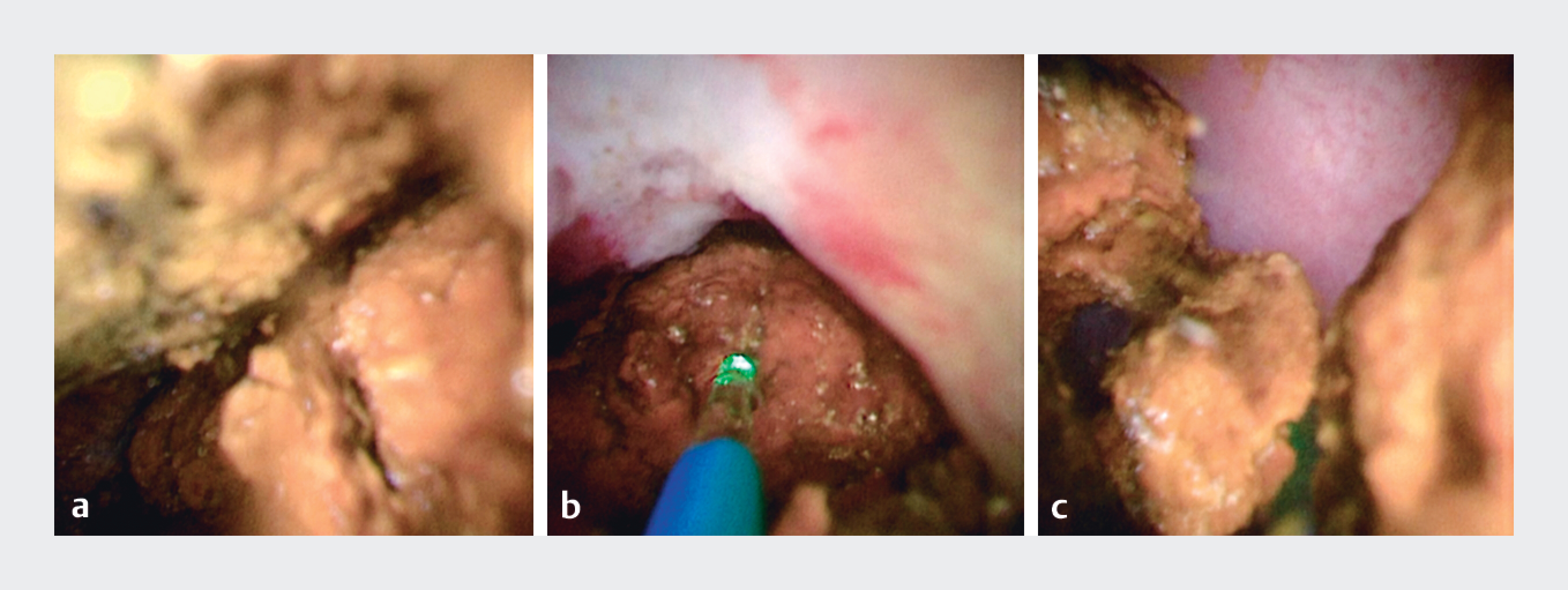
A 61-year-old woman with multiple large stones in the right intrahepatic bile duct, who had previously undergone hepaticojejunostomy with Roux-en-Y, was referred to us ([Fig. 2]). Endoscopic retrograde cholangiopancreatography was performed using a short-type single-balloon enteroscopy (SIF-H290; Olympus Marketing, Japan) with a working length of 152 cm and a working channel of 3.2 mm in diameter ([Video 1] [1] [2]). Cholangiography revealed multiple large stones in the right intrahepatic bile duct ([Fig. 3]). Subsequently, POCS was performed using a thin cholangioscope and revealed multiple large stones in the intrahepatic bile duct ([Fig. 4] a). A laser fiber was introduced, and POCS-guided laser lithotripsy was performed under a clear field of view. Precise targeting and fragmentation of the stones were achieved safely ([Fig. 4] b,c), resulting in complete stone extraction ([Fig. 5]).



This case highlights the utility of POCS-guided laser lithotripsy using a thin cholangioscope, even in the setting of balloon enteroscopy. Both the thin cholangioscope and the laser fiber can improve the success rate of stone extraction in such patients.
Endoscopy_UCTN_Code_TTT_1AR_2AH
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos.
Contributorsʼ Statement
Yuki Tanisaka: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. Shomei Ryozawa: Supervision, Writing – review & editing. Masafumi Mizuide: Supervision, Writing – review & editing. Akashi Fujita: Investigation, Writing – review & editing. Ryuichi Watanabe: Investigation, Writing – review & editing. Ryosuke Hamamura: Investigation, Writing – review & editing.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Tanisaka Y, Ryozawa S, Itoi T. et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy-assisted ERCP for altered anatomy: a multicenter cohort in Japan. Gastrointest Endosc 2022; 95: 310-318.e1
- 2 Tanisaka Y, Mizuide M, Fujita A. et al. Factors affecting complete stone extraction in the initial procedure in short type single-balloon enteroscopy-assisted endoscopic retrograde cholangiography for patients with Roux-en-Y gastrectomy. Scand J Gastroenterol 2022; 57: 1390-1396
- 3 Tanisaka Y, Ryozawa S, Mizuide M. et al. Cholangioscopy-guided guidewire insertion into the gallbladder using a novel thin cholangioscope under balloon enteroscopy in a patient with Roux-en-Y gastrectomy. Endoscopy 2025; 57: E1023-E1024
- 4 Veld JV, van Huijgevoort NCM, Boermeester MA. et al. A systematic review of advanced endoscopy-assisted lithotripsy for retained biliary tract stones: laser, electrohydraulic or extracorporeal shock wave. Endoscopy 2018; 50: 896-909
- 5 McCarty TR, Gulati R, Rustagi T. Efficacy and safety of peroral cholangioscopy with intraductal lithotripsy for difficult biliary stones: a systematic review and meta-analysis. Endoscopy 2021; 53: 110-122
Correspondence
Publication History
Article published online:
19 November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Tanisaka Y, Ryozawa S, Itoi T. et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy-assisted ERCP for altered anatomy: a multicenter cohort in Japan. Gastrointest Endosc 2022; 95: 310-318.e1
- 2 Tanisaka Y, Mizuide M, Fujita A. et al. Factors affecting complete stone extraction in the initial procedure in short type single-balloon enteroscopy-assisted endoscopic retrograde cholangiography for patients with Roux-en-Y gastrectomy. Scand J Gastroenterol 2022; 57: 1390-1396
- 3 Tanisaka Y, Ryozawa S, Mizuide M. et al. Cholangioscopy-guided guidewire insertion into the gallbladder using a novel thin cholangioscope under balloon enteroscopy in a patient with Roux-en-Y gastrectomy. Endoscopy 2025; 57: E1023-E1024
- 4 Veld JV, van Huijgevoort NCM, Boermeester MA. et al. A systematic review of advanced endoscopy-assisted lithotripsy for retained biliary tract stones: laser, electrohydraulic or extracorporeal shock wave. Endoscopy 2018; 50: 896-909
- 5 McCarty TR, Gulati R, Rustagi T. Efficacy and safety of peroral cholangioscopy with intraductal lithotripsy for difficult biliary stones: a systematic review and meta-analysis. Endoscopy 2021; 53: 110-122