

Subscribe to RSS
DOI: 10.1055/a-2737-2046
Associations between Pathogenic Germline Variants in BRCA and Non-Breast/Non-Ovarian Cancer Types in the German Population
Assoziationen zwischen pathogenen Keimbahnvarianten in BRCA1/2 und verschiedenen Tumorentitäten in der deutschen BevölkerungAuthors

Abstract
Introduction
Families with pathogenic germline variants (pv) in BRCA1/2 may have besides breast and ovarian cancer an elevated lifetime risk for other cancer types.
Material and Methods
Data and pedigree information from 1852 family members of 286 BRCA1/2 positive families were analyzed. Genetic testing was conducted between 2015 and 2017 at the HBOC center at Charité – Universitätsmedizin Berlin. Relative cancer risk (RR) was calculated by comparing observed cancer incidence with the expected incidence in the German population.
Results
BRCA1/2 positive families showed an elevated cancer risk for gastric and cervical cancer regardless of BRCA status. The relative risk of gastric cancer was higher in BRCA2 carriers compared to BRCA1 carriers (gBRCA1 RR 1.42; 95% CI: 0.65–2.69 vs. gBRCA2 RR 1.88; 95% CI: 0.75–3.87). Similarly, the relative risk for cervical cancer was also greater in BRCA2 carriers than in BRCA1 carriers (gBRCA1 RR 1.88; 95% CI: 0.69–4.09 vs. gBRCA2 RR 2.09; 95% CI: 0.56–5.35). Additionally, BRCA2 families showed an increased risk of pancreatic cancer (RR 1.56; 95% CI, 0.50 to 3.63). No significant associations were found for other cancer entities.
Conclusion
In the present study, an increased risk of gastrointestinal cancer was observed in German families with pathogenic BRCA1/2 variants, consistent with findings from previous research. Potential new associations with cervical cancer were also identified, warranting confirmation through large prospective studies. These findings highlight the importance of developing additional screening programs or preventive strategies for BRCA carriers, especially with regard to upper gastrointestinal tract malignancies.
Zusammenfassung
Einleitung
Pathogene Keimbahnvarianten (pV) in BRCA1/2 sind mit einem erhöhten Risiko für Mamma- und Ovarialkarzinome assoziiert. Mögliche Zusammenhänge mit einem gesteigerten Risiko für weitere Tumorentitäten werden ebenfalls vermutet.
Material und Methoden
Es wurden Daten von 1852 Familienmitgliedern aus 286 BRCA1/2-positiven Familien ausgewertet, die sich im Zeitraum von 2015 bis 2017 am HBOC-Zentrum der Charité – Universitätsmedizin Berlin vorgestellt hatten. Das relative Krebsrisiko (RR) wurde durch den Vergleich der beobachteten Krebsinzidenz in der Studienpopulation mit der erwarteten Inzidenz in der deutschen Allgemeinbevölkerung berechnet.
Ergebnisse
In BRCA1/2-positiven Familien zeigte sich ein erhöhtes Risiko für Magen- und Zervixkarzinome, unabhängig vom BRCA-Status. Das Risiko für ein Magenkarzinom war bei BRCA2-Träger*innen höher als bei BRCA1-Träger*innen (gBRCA1 RR = 1,42; 95%-KI 0,65–2,69 vs. gBRCA2 RR = 1,88; 95%-KI 0,75–3,87). Für Zervixkarzinome ergab sich ein ähnlicher Trend (gBRCA1 RR = 1,88; 95%-KI 0,69–4,09 vs. gBRCA2 RR = 2,09; 95%-KI 0,56–5,35). BRCA2-Familien zeigten zudem ein erhöhtes Risiko für Pankreaskarzinome (RR = 1,56; 95%-KI 0,50–3,63). Für andere Tumorentitäten ergaben sich keine signifikanten Assoziationen.
Schlussfolgerung
Pathogene BRCA-Varianten sind in der vorliegenden Studie mit einem erhöhten Risiko für gastrointestinale Tumoren in der deutschen Bevölkerung assoziiert. Diese Ergebnisse stimmen mit früheren Untersuchungen überein. Potenzielle Zusammenhänge mit einer erhöhten Inzidenz von Zervixkarzinomen sollten in größeren prospektiven Studien überprüft werden. Die Befunde unterstreichen die Bedeutung zusätzlicher Screening- und Präventionsstrategien für BRCA-Träger*innen, insbesondere im Hinblick auf Malignome des oberen Gastrointestinaltrakts.
Schlüsselwörter
BRCA1/2 - pathogene Keimbahnvarianten - gastrointestinale Malignome - Assoziation - PräventionIntroduction
Breast cancer susceptibility genes (BRCA1/BRCA2), tumor suppressor genes first described in 1994, play an important role in DNA damage repair. Family history (including type of cancer and age at first diagnosis) is an important indicator for recommending genetic analysis [1] [2]. Pathogenic germline variants (pv) in BRCA1 or 2 increase the susceptibility to breast and ovarian cancer [3] [4]. Women with a pv in BRCA1 or 2 have a lifetime risk of developing breast or ovarian cancer up to 54–78% depending on the BRCA status [5]. Therefore, an intensified screening program for breast cancer as well as recommendations for individualized risk management strategies have been established [6], including prophylactic surgeries [7] [8]. Although, the connection between pathogenic germline variants in BRCA1/2 and breast or ovarian cancer is obvious, associations with other cancer entities remain less clear
In former studies, an association between pv in BRCA and pancreatic cancer was suggested, with BRCA2 carriers exhibiting a higher lifetime risk than BRCA1 carriers [9] [10] [11]. Unfortunately, no standard cancer screening program for pancreatic cancer has been established, yet. The American Society for Gastrointestinal Endoscopy (ASGE) recommends annual screening with magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP) or endoscopic ultrasonography (EUS) for BRCA carriers regardless of family history. Recommendations of the National Comprehensive Cancer Network (NCCN) guidelines depend on family history and include MRCP or EUS. Furthermore, screening protocols differ in terms of methods and recommended intervals [12] [13]. In Germany, the guideline published in 2024 recommends pancreatic screening for BRCA1/2 carriers with a first-degree relative affected by pancreatic cancer. The screening should begin at age 50 or 10 years prior to the relative’s age at diagnosis and should include MRI/MRCP and/or EUS [14]. There are contradictory data about associations between pv in BRCA and colon cancer. A recent systematic review including 11 studies found no significantly increased risk of colorectal cancer in BRCA carriers (OR 1.03; p = 0.82) not even in subgroup analysis (BRCA1 and BRCA2) and after adjusting for age and gender [15]. Although, other studies suggested a higher colon cancer incidence in BRCA1 positive families up to a fivefold increased risk and independent of gender [9] [16] [17].
Even if previous studies found a slightly higher risk of squamous cell carcinoma of the skin in BRCA1/2 carriers [18] [19] no increase in malignant melanoma among people carrying pv in BRCA was reported [18] [19] [20] [21].
Differences in prostate cancer risk between BRCA1 and BRCA2 carriers have also been described. For example, men with pv in BRCA2 have an elevated lifetime risk of prostate cancer up to 34% [9], whereas men with pv in BRCA1 did not seem to have an elevated prostate cancer risk [9] [10] [11] [22].
Conflicting results have also been observed regarding cervical cancer: to date, several studies have not reported an association between pv in BRCA genes and cervical cancer in the literature [9] [19] [23]. Conversely, other studies have suggested that women with a pv in BRCA1 or 2 may have a slightly increased risk of developing cervical cancer [21] [22], potentially due to alterations in the cervical microbiome [24].
An increasing incidence of gastric cancer has been suggested in previous studies [9] [10] [19]. In a recent review by Buckley et al., the lifetime cumulative risk of gastric cancer was up to 19.3% in BRCA2 carriers, whereas BRCA1 families had a likely increased risk [25]. Furthermore, Usui et al. described an association between pv in BRCA1/2, Helicobacter pylori infection and gastric cancer risk [26].
The present study aims to analyze the incidence of non-breast and non-ovarian cancer entities in carriers of pathogenic BRCA germline variants in comparison to the general population. To our knowledge, this is one of few studies to analyze the cancer spectrum associated with pv in BRCA outside of breast and ovarian cancer specifically in the German population [27].
Material and Methods
Study design and population
This retrospective cohort study was conducted at Hereditary Breast and Ovarian Cancer Center Charité – Universitätsmedizin Berlin, Germany (HBOCC). Ethics approval was granted by the ethics committee of Charité – Universitätsmedizin Berlin (EA1/287/19).
The study included individuals who underwent genetic counseling at HBOCC between 2015 and 2017 – either as healthy individuals with a family history of cancer or as patients diagnosed with breast and/or ovarian cancer, often with an additional family history of cancer – and shown pathogenic germline variants in BRCA1/2. Participants were excluded if they carried a pv in any other gene than BRCA1/2. Furthermore, all individuals had to be at least 18 years old and provided informed consent to participate in clinical trials. All first-, second- and third-degree relatives of these individuals were included anonymously in the study. Family members were excluded if gender, age or type of cancer diagnosis was unknown.
Data collection
Characteristics like date of birth, age at time of death, pv, number of cancers, cancer type, and age at diagnosis were obtained from individuals counseled at HBOCC for herself and family members across three generations. All data was based on self-reports provided by the counselee. To identify the parental side affected by the pathogenic germline variant, self-reported information on genetic testing of family members as well as incidences of breast and ovarian cancer was used. The parental line in which these cancers predominantly occurred was defined as the BRCA positive line. Families were excluded if identification of the parental line was not possible.
We focused our investigation on gastric, pancreatic, colon, as well as prostate, uterine and cervical cancers and malignant melanoma. The incidence of these cancer types in the genetic parental line was calculated based on information given by the index patient of the family.
Statistical analysis
The relative risk (RR) was estimated by comparing the observed cancer incidence with the expected incidence. To calculate the expected incidence we used the average cancer incidence per 100000 residents as reported by the Robert Koch Institute (RKI) [28]. To measure the confidence intervals the Byar’s approximation of the exact poisson distribution was used [29]. Statistical analyses were performed by using IBM SPSS Statistics 26.0.
Initially, we aimed to include 350 index patients each with an average of approximately eight family members, resulting in an expected total of 2700 to 3000 individuals. For planning we assumed a total of 10 to 100 absolute cancer occurrences of a certain type. Based on this, we calculated 95% confidence interval (95% CI) widths for the RR, ranging from 0.25 to 2.0. The 95%-CI-widths were below 1.9 for 10 occurrences, below 1.3 for 20 occurrences, and below 1.0 for all other numbers. This level of precision was considered sufficient for the analysis of these rare cancers. Sample size justification was done using R [29].
Results
Study cohort
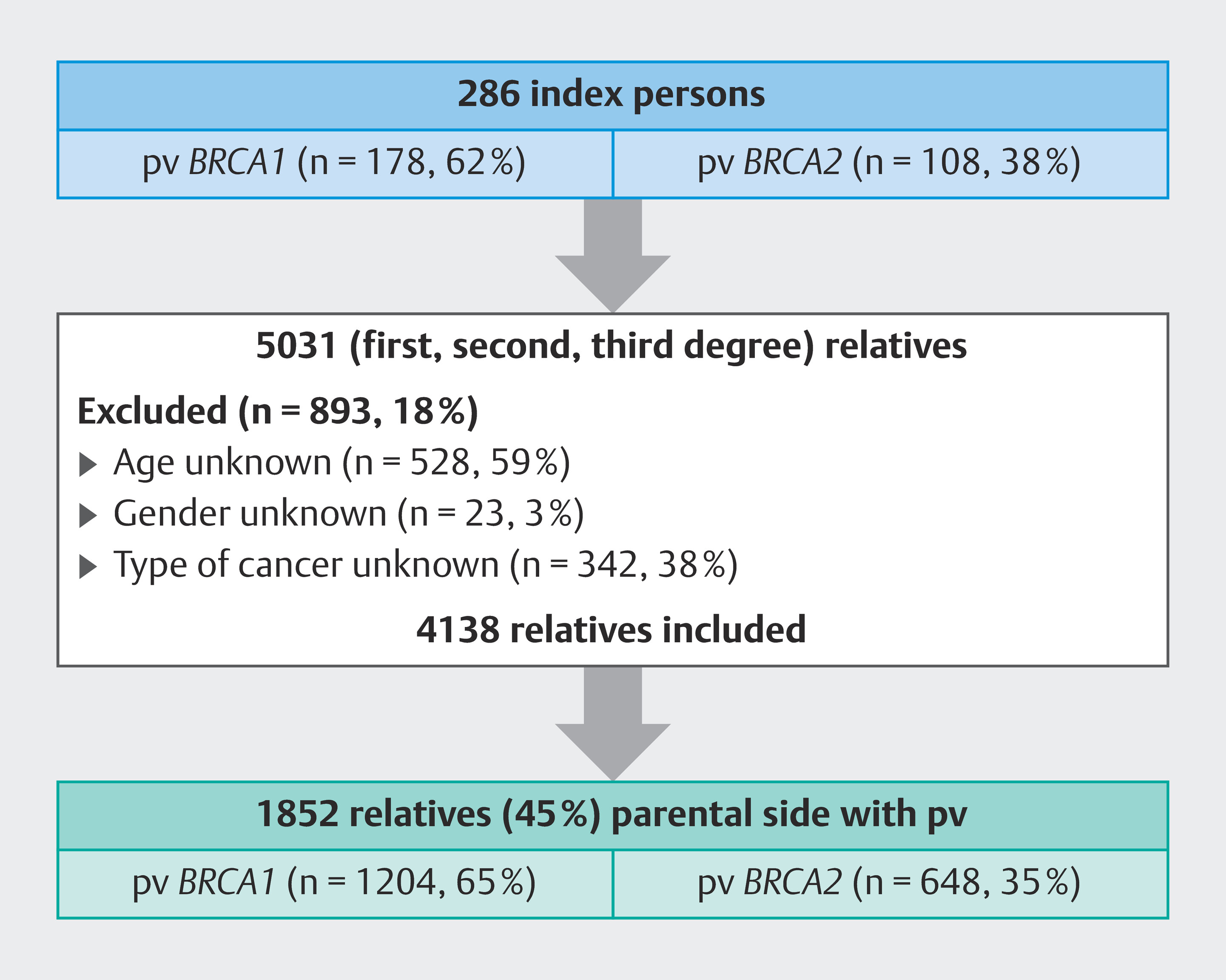
Between 2015–2017, pathogenic germline variants in BRCA1/2 were detected in 286 index persons at HBOCC, who had previously given their consent to participate in clinical trials. The majority of cases tested positive for BRCA1 (n = 178/286, 62%), while 38% (n= 108/286) carried pathogenic variants in BRCA2. Pedigrees of these index persons included information on 5031 relatives, of whom 4138 (82%) could be included in the study comprising 2376 women (57%) and 1762 men (43%). A total of 893 individuals (18%) were excluded due to missing information on birth year, current age, or cancer diagnoses.
In the present study, we focused on the parental side from which the pathogenic germline variant was inherited. Overall, 1852 of the 4138 relatives (45%) could be identified to these parental lines. Most individuals belonged to BRCA1 families (n = 1204/1852; 65%). The study population is illustrated in [Fig. 1].
Cancer characteristics in counselees
Most female counselees had breast cancer (n = 142/273; 52%) while 25% reported a history of ovarian cancer (n = 72/273) and 20% had never been diagnosed with cancer (n = 56/273). This was independent of BRCA status. In the study two male counselees reported a history of breast cancer. The occurrence of breast and ovarian cancer in counselees in accordance to BRCA status is shown in [Table 1] and illustrated in [Fig. 2].

The following results describe the incidence of specific cancer types in the genetically impacted parental lineage compared to the general German population. These data is demonstrated in [Table 2].
Gastrointestinal cancers
Regarding gastrointestinal cancer occurrence in BRCA1 families the observed incidence of gastric cancer was higher than expected when compared to the general population (RR 1.42; 95% CI 0.65–2.69). In contrast, no increased relative risk was observed for either colorectal or pancreatic cancer in BRCA1 carriers.
Conversely, potential associations between pathogenic variants in BRCA2 and gastrointestinal cancer were observed. Notably, the relative risk for gastric cancer was higher in BRCA2 carriers (RR 1.88; 95% CI 0.75–3.87) compared to those in BRCA1 families (RR 1.42; 95% CI 0.65–2.69). Additionally, a trend toward an increased risk of pancreatic cancer was identified in individuals from families with pathogenic BRCA2 variants (RR 1.56; 95% CI 0.50–3.63), which was higher than the corresponding risk observed in BRCA1 families. In contrast, no association between colon cancer and BRCA2 carriers was found.
Gynecologic cancers
Furthermore, women from families with pathogenic BRCA1 variants appeared to have a higher incidence of cervical cancer (RR 1.88; 95% CI 0.69–4.09). A similar tendency was noted in BRCA2-positive families, where women harboring pathogenic variants in BRCA2 showed approximately a twofold increase in incidence (RR 2.09; 95% CI 0.56–5.35).
Prostate cancer and malignant melanoma
There was no increased relative risk of prostate cancer in any of the families. Nevertheless, BRCA2 carriers showed a higher relative risk of prostate cancer compared to BRCA1 carriers (pv BRCA1 RR 0.57; 95% CI 0.29–1.04; pv BRCA2 RR 0.67; 95% CI 0.27–1.37).
Similarly, the incidence of malignant melanoma was not elevated in either group.
Age at cancer diagnosis
To investigate potential differences in cancer onset, we compared the age at diagnosis between the study population and the general population across several cancer types ([Table 1], [Table 2], [Table 3]). In all cancer types analyzed, patients in the study population were diagnosed at a younger age. This trend was particularly evident for upper gastrointestinal cancers. For example, the mean age at diagnosis for pancreatic cancer was 65 years in the study population compared to 74 years in the general population. Similarly, cervical cancer was diagnosed approximately a decade earlier in the study group [28].
Discussion
The growing importance of genomic medicine, combined with recent scientific progress, has led to a significant expansion of knowledge about the breast and ovarian cancer risks associated to pathogenic variants in BRCA1/2. To optimize risk management, effective preventive strategies have been developed over time.
In contrast, data on the association between pathogenic variants in BRCA and the incidence of cancer types other than breast and ovarian cancer, particularly within the German population, remain limited. This uncertainty contributes to gaps in preventive strategies, resulting in an inadequate level of patient care.
In the present study, a total of 286 index cases and 4138 relatives were included. Among these, 1852 individuals belonged to the genetically affected line and underwent analysis. As the focus of risk assessment was on the BRCA-positive line, our study population consisted exclusively of members from the genetically affected line. This sample size is comparable to that of other single-center studies [18] [22]. Nevertheless, it was slightly lower than the previously expected needed number of index cases. The majority of index cases in the present study were found to have a pv in BRCA1 (62%), while 38% exhibited a pv in BRCA2. A previous large-scale study examined the prevalence of pv in BRCA among 21401 German families and reported similar findings for the tested index cases, with a higher occurrence of BRCA1 (16% vs. 8% BRCA2) [30].
In our study women with pv in BRCA1 reported more breast and ovarian cancer than BRCA2 carriers, similar to other studies [31] [32]. Furthermore, two men in our cohort had a history of breast cancer each with a pv in BRCA1 or BRCA2. In contrast, literature suggests that the risk of male breast cancer seemed to be higher in BRCA2 carriers compared to BRCA1 [33].
In summary, only 18 male index cases (4%) and 85 male unaffected relatives (12%) underwent genetic testing in our study. The limited number of male participants may partly explain the low incidence of breast cancer among men with pv in BRCA1/2. Additionally, the low testing rate highlights the urgent need to enhance awareness regarding the association between pv in BRCA and cancer risks in men. For instance, Thomas et al. reported that 80% of men did not express concern about breast cancer, despite having a positive family history [34]. Despite eligibility, men are less often referred for BRCA testing, and among those referred, completion rates remain lower than in women [35]. Furthermore, there are currently no standardized screening recommendations for high-risk men [36], even though literature indicates an increased incidence of breast cancer in this population [33].
A major finding of our study was the indication of a potentially increased risk for gastrointestinal cancer in BRCA carriers, particularly in BRCA2 families. To date, a limitation of the following findings described in the present study are the wide ranges of the 95%-confidence intervals.
We observed a statistic trend towards an increased risk of gastric cancer in BRCA carriers, with the highest relative risk seen in families with pv in BRCA2 [37]. Other studies also suggested an association between pv in BRCA and risk for gastric cancer, especially in BRCA2 carriers [9] [10] [16] [19]. Schlebusch et al. reported that BRCA2 carriers had twice the risk of gastric cancer risk than BRCA1 carriers [23].
Furthermore, our analyses did not indicate an association between pancreatic cancer and BRCA1 families. This finding is similar to previous studies [19] [22], although other studies have suggested a slightly increased risk of pancreatic cancer in BRCA1 carriers [9] [10] [11]. On the other hand, our data suggested a possible association between pv in BRCA2 and elevated pancreatic cancer risk. However, the estimated relative risk of pancreatic cancer in our study (RR 1.56) appeared to be lower than the risk reported in earlier studies, with estimated relative risks ranging from 3 to 6 [9] [11] [19] [38]. Despite this, pancreatic cancer was more common in BRCA2 carriers in our cohort consistent with previous research [9] [10] [11] [19] [22]. Importantly, the 5-year surveillance rate of pancreatic cancer ranged between 3.1–6.1% in BRCA families in previous studies. Most died within the first year after diagnosis [39]. However, in a recently published study by Blackford et al. pancreatic cancer surveillance by EUS or MRI lead to lower-stage pancreatic cancer and a higher overall survival rate [40]. This indicates that an enhanced screening program for pancreatic cancer is long overdue, particularly for BRCA2 carriers. Although the German guideline recommends a screening program for BRCA1/2 carriers [14], there is a lack of certified centers and structured programs regarding type and frequency of screening. This highlights the need of standardized guidelines for pancreatic cancer screening especially in high-risk groups. Moreover, current genetic testing criteria for BRCA mutations focus solely on a family history of breast and ovarian cancer [41], while cases of pancreatic cancer are not considered. Since associations with pancreatic cancer and other cancer types are assumed, an expansion of the testing criteria should be considered to improve the patient centered care of high-risk groups.
In our study, no association was identified between pv in BRCA1 and prostate cancer, which is consistent with the majority of previous studies [9] [22] [23] [42]. Although the literature reports an increased incidence of prostate cancer among BRCA2 carriers [9] [10] [11] [19] [22] [38], no elevated prostate cancer risk was seen in our cohort. This low incidence may be partly explained by the limited participation of German men in prostate cancer screening programs—only 12% underwent screening [43]. Participation rates tend to increase with age; however, the majority of men in our study were younger than 60 years of age. Our findings underscore the necessity of enhancing awareness of prostate cancer, particularly among BRCA2 carriers, to improve participation in screening programs.
A slightly increased risk of cervical cancer was identified among BRCA1/2 carriers within the analyzed patient population. While previous studies reported no significant association [9] [19] [23], some authors documented an elevated incidence of cervical cancer in BRCA carriers [21] [22]. In our study, the risk of cervical cancer was notably higher in women with pv in BRCA2 compared to those with pv in BRCA1. These findings are consistent with those reported by Mersch et al., who observed a significant trend indicating an increased incidence of cervical cancer in BRCA2 carriers relative to the general population (p = 0.006) [22].
An infection with human papillomavirus (HPV) is the most common cause of cervical cancer [44]. The association between BRCA and HPV infection is poorly understood whereas a higher prevalence of high-risk HPV types in women with familial breast cancer was described in the literature [45].
Additionally, a review by Liu et al. suggested that dysfunction in BRCA may lead to unregulated cellular proliferation driven by oncogenes such as E6/E7, potentially increasing the risk of cervical cancer [46]. Furthermore, BRCA1 carriers were more likely to have a cervicovaginal microbiome characterized by a predominance of less than 50% lactobacilli species [24], which is thought to play a critical role in the pathogenesis of cervical cancer [47]. The proposed association warrants further investigation in future studies.
In our study, the average age at cancer diagnosis was consistently lower than in the general German population [28]. The difference was particularly notable for upper gastrointestinal cancers, such as gastric and pancreatic cancer, which were diagnosed nearly a decade earlier in the study population. Similar findings have been reported for both BRCA1 and BRCA2 carriers indicating a higher risk of early-onset cancer in the literature [21] [38]. This supports the implementation of risk-adapted, early detection strategies.
Our study has several limitations. The retrospective design and reliance on self-reported cancer histories may have led to data gaps and an underestimation of the incidence of certain cancer types. In some cases, the specific cancer diagnosis in affected ancestors was unclear or could not be reliably determined; such cases were excluded from the analysis. Pathological confirmation of reported cancers would help to mitigate this source of error. Additionally, in approximately one third of the families, it was not possible to ascertain the paternal lineage. Because the study population was smaller than expected, this may have limited the statistical power and led to confidence intervals that were occasionally wider. The clinically relevant associations observed in our study should therefore be confirmed in future research using larger study populations. We also did not account for potential confounders such as lifestyle factors and socioeconomic status. These unmeasured variables may influence cancer risk and could potentially bias the observed associations.
Furthermore, we compared the cancer incidence in our cohort with that of the general German population as reported by RKI. Comparing the study population with a control group matched for age and gender could reduce possible error.
The strengths of our study include the comprehensive data collection spanning at least three generations and the substantial sample size for a single-center investigation. Despite the limitations, our study findings are largely consistent with those of previous large-scale studies and thus reinforce the observed associations within the German population.
Conclusion
In summary, our study suggests an increased risk of cervical cancer in BRCA carriers which warrants further exploration in future clinical research. Additionally, we observed an association between pathogenic germline variants in BRCA2 and an elevated risk of pancreatic cancer, as well as between pathogenic germline variants in BRCA1/2 and gastric cancer risk. These findings underscore the urgent need for improved screening strategies for upper gastrointestinal cancers to enhance clinical care and outcomes for BRCA mutation carriers.
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgement
We thank Ramona Peters for her excellent help with data collection and analysis.
-
References
- 1 Couch FJ. Genetic epidemiology of BRCA1. Cancer Biol Ther 2004; 3: 509-514
- 2 Kwong A, Cheuk IW, Shin VY. et al. Somatic mutation profiling in BRCA-negative breast and ovarian cancer patients by multigene panel sequencing. Am J Cancer Res 2020; 10: 2919-2932
- 3 Miki Y, Swensen J, Shattuck-Eidens D. et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994; 266: 66-71
- 4 Wooster R, Bignell G, Lancaster J. et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995; 378: 789-792
- 5 Antoniou A, Pharoah PD, Narod S. et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 2003; 72: 1117-1130
- 6 Bick U. [High-risk screening using magnetic resonance imaging]. Radiologe 2021; 61: 150-158
- 7 Lorenz J. Risikoreduzierende Chirurgie bei BRCA-Mutationsträgerinnen. Geburtshilfe Frauenheilkd 2025; 85: 898
- 8 Meindl A, Ditsch N, Kast K. et al. Hereditary breast and ovarian cancer: new genes, new treatments, new concepts. Dtsch Arztebl Int 2011; 108: 323-330
- 9 Li S, Silvestri V, Leslie G. et al. Cancer Risks Associated With BRCA1 and BRCA2 Pathogenic Variants. J Clin Oncol 2022; 40: 1529-1541
- 10 Momozawa Y, Sasai R, Usui Y. et al. Expansion of Cancer Risk Profile for BRCA1 and BRCA2 Pathogenic Variants. JAMA Oncol 2022; 8: 871-878
- 11 Risch HA, McLaughlin JR, Cole DE. et al. Population BRCA1 and BRCA2 mutation frequencies and cancer penetrances: a kin-cohort study in Ontario, Canada. J Natl Cancer Inst 2006; 98: 1694-1706
- 12 FORCE-Facing Our Risk of Cancer Empowered. Pancreatic Cancer Screening Guidelines. Accessed December 15, 2024 at: https://www.facingourrisk.org/info/risk-management-and-treatment/screening-and-risk-reduction/by-cancer-type/pancreatic/guidelines%23:~:text=All%20people%20with%20a%20BRCA1,pancreatic%20cancer%20in%20the%20family
- 13 Partyka O, Pajewska M, Kwaśniewska D. et al. Overview of Pancreatic Cancer Epidemiology in Europe and Recommendations for Screening in High-Risk Populations. Cancers (Basel) 2023; 15: 3571
- 14 Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF). S3-Leitlinie Exokrines Pankreaskarzinom, Langversion 3.1, AWMFRegisternummer: 032–010OL. 2024 Accessed December 15, 2024 at: https://www.leitlinienprogrammonkologie.de/leitlinien/pankreaskarzinom/
- 15 Cullinane CM, Creavin B, O’Connell EP. et al. Risk of colorectal cancer associated with BRCA1 and/or BRCA2 mutation carriers: systematic review and meta-analysis. Br J Surg 2020; 107: 951-959
- 16 Fasching P, Lux M, Bani M. et al. Hereditäres Mamma- und Ovarialkarzinom – ein Update Teil I – molekulare Grundlagen, Tumorrisikoberatung und Risikoberechnung. Geburtshilfe Frauenheilkd 2004; 64: 900-911
- 17 Sopik V, Phelan C, Cybulski C. et al. BRCA1 and BRCA2 mutations and the risk for colorectal cancer. Clin Genet 2015; 87: 411-418
- 18 Johannsson O, Loman N, Möller T. et al. Incidence of malignant tumours in relatives of BRCA1 and BRCA2 germline mutation carriers. Eur J Cancer 1999; 35: 1248-1257
- 19 Moran A, O’Hara C, Khan S. et al. Risk of cancer other than breast or ovarian in individuals with BRCA1 and BRCA2 mutations. Fam Cancer 2012; 11: 235-242
- 20 Brose MS, Rebbeck TR, Calzone KA. et al. Cancer risk estimates for BRCA1 mutation carriers identified in a risk evaluation program. J Natl Cancer Inst 2002; 94: 1365-1372
- 21 Thompson D, Easton DF. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 2002; 94: 1358-1365
- 22 Mersch J, Jackson MA, Park M. et al. Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer 2015; 121: 269-275
- 23 Schlebusch CM, Dreyer G, Sluiter MD. et al. Cancer prevalence in 129 breast-ovarian cancer families tested for BRCA1 and BRCA2 mutations. S Afr Med J 2010; 100: 113-117
- 24 Nené NR, Reisel D, Leimbach A. et al. Association between the cervicovaginal microbiome, BRCA1 mutation status, and risk of ovarian cancer: a case-control study. Lancet Oncol 2019; 20: 1171-1182
- 25 Buckley KH, Niccum BA, Maxwell KN. et al. Gastric Cancer Risk and Pathogenesis in BRCA1 and BRCA2 Carriers. Cancers (Basel) 2022; 14: 5816
- 26 Usui Y, Taniyama Y, Endo M. et al. Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer. N Engl J Med 2023; 388: 1181-1190
- 27 Bosse K. Assoziierte Tumoren in 266 Familien mit einer nachgewiesenen BRCA1/2 Mutation bzw. hohen Wahrscheinlichkeit für ein anderes autosomal dominantes Hochrisikogen. Zentralbl Gynakol 2005; 127: P2_11
- 28 Robert Koch-Institut (Hrsg.), Gesellschaft der epidemiologischen Krebsregister in Deutschland e. V. (Hrsg.). Krebs in Deutschland für 2015/2016. 12. Ausgabe. und die Berlin: Robert Koch-Institut; 2019
- 29 Breslow NE, Day NE. Statistical methods in cancer research. Volume II--The design and analysis of cohort studies. IARC Sci Publ 1987; 1987: 1-406
- 30 Kast K, Rhiem K, Wappenschmidt B. et al. Prevalence of BRCA1/2 germline mutations in 21 401 families with breast and ovarian cancer. J Med Genet 2016; 53: 465-471
- 31 Engel C, Fischer C, Zachariae S. et al. Breast cancer risk in BRCA1/2 mutation carriers and noncarriers under prospective intensified surveillance. Int J Cancer 2020; 146: 999-1009
- 32 Kuchenbaecker KB, Hopper JL, Barnes DR. et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017; 317: 2402-2416
- 33 Tai YC, Domchek S, Parmigiani G. et al. Breast cancer risk among male BRCA1 and BRCA2 mutation carriers. J Natl Cancer Inst 2007; 99: 1811-1814
- 34 Thomas E. Original Research: Men’s awareness and knowledge of male breast cancer. Am J Nurs 2010; 110: 32-37 9–40; quiz 1–2
- 35 Smith W, Smith K, Sessions W, Evins C, Baker M, Blumer M. An Evaluation of Gender Discrepancies in genetic Referrals for BRCA Testing for indicated Malignancies. Riverwoods, IL: Wolters Kluwer Health; 2021
- 36 Gaddam S, Heller SL, Babb JS. et al. Male Breast Cancer Risk Assessment and Screening Recommendations in High-Risk Men Who Undergo Genetic Counseling and Multigene Panel Testing. Clin Breast Cancer 2021; 21: e74-e79
- 37 Kim H, Choi DH, Park W. et al. The association between non-breast and ovary cancers and BRCA mutation in first- and second-degree relatives of high-risk breast cancer patients: a large-scale study of Koreans. Hered Cancer Clin Pract 2019; 17: 1
- 38 van Asperen CJ, Brohet RM, Meijers-Heijboer EJ. et al. Cancer risks in BRCA2 families: estimates for sites other than breast and ovary. J Med Genet 2005; 42: 711-719
- 39 Iqbal J, Ragone A, Lubinski J. et al. The incidence of pancreatic cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer 2012; 107: 2005-2009
- 40 Blackford AL, Canto MI, Dbouk M. et al. Pancreatic Cancer Surveillance and Survival of High-Risk Individuals. JAMA Oncol 2024; 10: 1087-1096
- 41 DKG. Zertifizierung der Deutschen Krebsgesellschaft Dokumente. Accessed January 23, 2025 at: https://www.krebsgesellschaft.de/zertdokumente.html
- 42 Fachal L, Gómez-Caamaño A, Celeiro-Muñoz C. et al. BRCA1 mutations do not increase prostate cancer risk: results from a meta-analysis including new data. Prostate 2011; 71: 1768-1779
- 43 Grobe TG, Steinmann S, Szecsenyi J. Barmer Arztreport 2019. Schriftenreihe zur Gesundheitsanalyse. Berlin: Barmer; 2019
- 44 Guan P, Howell-Jones R, Li N. et al. Human papillomavirus types in 115,789 HPV-positive women: a meta-analysis from cervical infection to cancer. Int J Cancer 2012; 131: 2349-2359
- 45 Mohtasebi P, Rassi H, Maleki F. et al. Detection of Human Papillomavirus Genotypes and Major BRCA Mutations in Familial Breast Cancer. Monoclon Antib Immunodiagn Immunother 2016; 35: 135-140
- 46 Liu GB, Chen J, Wu ZH. et al. Association of human papillomavirus with Fanconi anemia promotes carcinogenesis in Fanconi anemia patients. Rev Med Virol 2015; 25: 345-353
- 47 Santella B, Schettino MT, Franci G. et al. Microbiota and HPV: The role of viral infection on vaginal microbiota. J Med Virol 2022; 94: 4478-4484
Correspondence
Publication History
Received: 06 July 2025
Accepted after revision: 29 October 2025
Article published online:
28 November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Couch FJ. Genetic epidemiology of BRCA1. Cancer Biol Ther 2004; 3: 509-514
- 2 Kwong A, Cheuk IW, Shin VY. et al. Somatic mutation profiling in BRCA-negative breast and ovarian cancer patients by multigene panel sequencing. Am J Cancer Res 2020; 10: 2919-2932
- 3 Miki Y, Swensen J, Shattuck-Eidens D. et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994; 266: 66-71
- 4 Wooster R, Bignell G, Lancaster J. et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995; 378: 789-792
- 5 Antoniou A, Pharoah PD, Narod S. et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 2003; 72: 1117-1130
- 6 Bick U. [High-risk screening using magnetic resonance imaging]. Radiologe 2021; 61: 150-158
- 7 Lorenz J. Risikoreduzierende Chirurgie bei BRCA-Mutationsträgerinnen. Geburtshilfe Frauenheilkd 2025; 85: 898
- 8 Meindl A, Ditsch N, Kast K. et al. Hereditary breast and ovarian cancer: new genes, new treatments, new concepts. Dtsch Arztebl Int 2011; 108: 323-330
- 9 Li S, Silvestri V, Leslie G. et al. Cancer Risks Associated With BRCA1 and BRCA2 Pathogenic Variants. J Clin Oncol 2022; 40: 1529-1541
- 10 Momozawa Y, Sasai R, Usui Y. et al. Expansion of Cancer Risk Profile for BRCA1 and BRCA2 Pathogenic Variants. JAMA Oncol 2022; 8: 871-878
- 11 Risch HA, McLaughlin JR, Cole DE. et al. Population BRCA1 and BRCA2 mutation frequencies and cancer penetrances: a kin-cohort study in Ontario, Canada. J Natl Cancer Inst 2006; 98: 1694-1706
- 12 FORCE-Facing Our Risk of Cancer Empowered. Pancreatic Cancer Screening Guidelines. Accessed December 15, 2024 at: https://www.facingourrisk.org/info/risk-management-and-treatment/screening-and-risk-reduction/by-cancer-type/pancreatic/guidelines%23:~:text=All%20people%20with%20a%20BRCA1,pancreatic%20cancer%20in%20the%20family
- 13 Partyka O, Pajewska M, Kwaśniewska D. et al. Overview of Pancreatic Cancer Epidemiology in Europe and Recommendations for Screening in High-Risk Populations. Cancers (Basel) 2023; 15: 3571
- 14 Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF). S3-Leitlinie Exokrines Pankreaskarzinom, Langversion 3.1, AWMFRegisternummer: 032–010OL. 2024 Accessed December 15, 2024 at: https://www.leitlinienprogrammonkologie.de/leitlinien/pankreaskarzinom/
- 15 Cullinane CM, Creavin B, O’Connell EP. et al. Risk of colorectal cancer associated with BRCA1 and/or BRCA2 mutation carriers: systematic review and meta-analysis. Br J Surg 2020; 107: 951-959
- 16 Fasching P, Lux M, Bani M. et al. Hereditäres Mamma- und Ovarialkarzinom – ein Update Teil I – molekulare Grundlagen, Tumorrisikoberatung und Risikoberechnung. Geburtshilfe Frauenheilkd 2004; 64: 900-911
- 17 Sopik V, Phelan C, Cybulski C. et al. BRCA1 and BRCA2 mutations and the risk for colorectal cancer. Clin Genet 2015; 87: 411-418
- 18 Johannsson O, Loman N, Möller T. et al. Incidence of malignant tumours in relatives of BRCA1 and BRCA2 germline mutation carriers. Eur J Cancer 1999; 35: 1248-1257
- 19 Moran A, O’Hara C, Khan S. et al. Risk of cancer other than breast or ovarian in individuals with BRCA1 and BRCA2 mutations. Fam Cancer 2012; 11: 235-242
- 20 Brose MS, Rebbeck TR, Calzone KA. et al. Cancer risk estimates for BRCA1 mutation carriers identified in a risk evaluation program. J Natl Cancer Inst 2002; 94: 1365-1372
- 21 Thompson D, Easton DF. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 2002; 94: 1358-1365
- 22 Mersch J, Jackson MA, Park M. et al. Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer 2015; 121: 269-275
- 23 Schlebusch CM, Dreyer G, Sluiter MD. et al. Cancer prevalence in 129 breast-ovarian cancer families tested for BRCA1 and BRCA2 mutations. S Afr Med J 2010; 100: 113-117
- 24 Nené NR, Reisel D, Leimbach A. et al. Association between the cervicovaginal microbiome, BRCA1 mutation status, and risk of ovarian cancer: a case-control study. Lancet Oncol 2019; 20: 1171-1182
- 25 Buckley KH, Niccum BA, Maxwell KN. et al. Gastric Cancer Risk and Pathogenesis in BRCA1 and BRCA2 Carriers. Cancers (Basel) 2022; 14: 5816
- 26 Usui Y, Taniyama Y, Endo M. et al. Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer. N Engl J Med 2023; 388: 1181-1190
- 27 Bosse K. Assoziierte Tumoren in 266 Familien mit einer nachgewiesenen BRCA1/2 Mutation bzw. hohen Wahrscheinlichkeit für ein anderes autosomal dominantes Hochrisikogen. Zentralbl Gynakol 2005; 127: P2_11
- 28 Robert Koch-Institut (Hrsg.), Gesellschaft der epidemiologischen Krebsregister in Deutschland e. V. (Hrsg.). Krebs in Deutschland für 2015/2016. 12. Ausgabe. und die Berlin: Robert Koch-Institut; 2019
- 29 Breslow NE, Day NE. Statistical methods in cancer research. Volume II--The design and analysis of cohort studies. IARC Sci Publ 1987; 1987: 1-406
- 30 Kast K, Rhiem K, Wappenschmidt B. et al. Prevalence of BRCA1/2 germline mutations in 21 401 families with breast and ovarian cancer. J Med Genet 2016; 53: 465-471
- 31 Engel C, Fischer C, Zachariae S. et al. Breast cancer risk in BRCA1/2 mutation carriers and noncarriers under prospective intensified surveillance. Int J Cancer 2020; 146: 999-1009
- 32 Kuchenbaecker KB, Hopper JL, Barnes DR. et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017; 317: 2402-2416
- 33 Tai YC, Domchek S, Parmigiani G. et al. Breast cancer risk among male BRCA1 and BRCA2 mutation carriers. J Natl Cancer Inst 2007; 99: 1811-1814
- 34 Thomas E. Original Research: Men’s awareness and knowledge of male breast cancer. Am J Nurs 2010; 110: 32-37 9–40; quiz 1–2
- 35 Smith W, Smith K, Sessions W, Evins C, Baker M, Blumer M. An Evaluation of Gender Discrepancies in genetic Referrals for BRCA Testing for indicated Malignancies. Riverwoods, IL: Wolters Kluwer Health; 2021
- 36 Gaddam S, Heller SL, Babb JS. et al. Male Breast Cancer Risk Assessment and Screening Recommendations in High-Risk Men Who Undergo Genetic Counseling and Multigene Panel Testing. Clin Breast Cancer 2021; 21: e74-e79
- 37 Kim H, Choi DH, Park W. et al. The association between non-breast and ovary cancers and BRCA mutation in first- and second-degree relatives of high-risk breast cancer patients: a large-scale study of Koreans. Hered Cancer Clin Pract 2019; 17: 1
- 38 van Asperen CJ, Brohet RM, Meijers-Heijboer EJ. et al. Cancer risks in BRCA2 families: estimates for sites other than breast and ovary. J Med Genet 2005; 42: 711-719
- 39 Iqbal J, Ragone A, Lubinski J. et al. The incidence of pancreatic cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer 2012; 107: 2005-2009
- 40 Blackford AL, Canto MI, Dbouk M. et al. Pancreatic Cancer Surveillance and Survival of High-Risk Individuals. JAMA Oncol 2024; 10: 1087-1096
- 41 DKG. Zertifizierung der Deutschen Krebsgesellschaft Dokumente. Accessed January 23, 2025 at: https://www.krebsgesellschaft.de/zertdokumente.html
- 42 Fachal L, Gómez-Caamaño A, Celeiro-Muñoz C. et al. BRCA1 mutations do not increase prostate cancer risk: results from a meta-analysis including new data. Prostate 2011; 71: 1768-1779
- 43 Grobe TG, Steinmann S, Szecsenyi J. Barmer Arztreport 2019. Schriftenreihe zur Gesundheitsanalyse. Berlin: Barmer; 2019
- 44 Guan P, Howell-Jones R, Li N. et al. Human papillomavirus types in 115,789 HPV-positive women: a meta-analysis from cervical infection to cancer. Int J Cancer 2012; 131: 2349-2359
- 45 Mohtasebi P, Rassi H, Maleki F. et al. Detection of Human Papillomavirus Genotypes and Major BRCA Mutations in Familial Breast Cancer. Monoclon Antib Immunodiagn Immunother 2016; 35: 135-140
- 46 Liu GB, Chen J, Wu ZH. et al. Association of human papillomavirus with Fanconi anemia promotes carcinogenesis in Fanconi anemia patients. Rev Med Virol 2015; 25: 345-353
- 47 Santella B, Schettino MT, Franci G. et al. Microbiota and HPV: The role of viral infection on vaginal microbiota. J Med Virol 2022; 94: 4478-4484