

Subscribe to RSS
DOI: 10.1055/a-2719-8908
Exploring the Etiologies of Acquired Unilateral Proptosis: A Literature Review with Case Presentations
Authors
Funding Information This study was supported by the research fund of the Dankook University, 2024.
Abstract
Acquired unilateral proptosis is a clinically significant condition with diverse etiologies, including trauma, inflammation or infection, tumors, and hemodynamic complications. This study aimed to improve recognition by integrating a literature review with illustrative case reports. Four representative cases were described, covering orbital infection, traumatic hematoma, carotid–cavernous fistula, and metastatic tumor. A focused literature review of publications from 2020 to 2024 was conducted, identifying 338 relevant studies, of which 171 met the inclusion criteria. Among the 171 eligible studies analyzed, tumors were the most frequent cause (93/171, 54.4%), followed by hemodynamic disorders (24/171, 14.0%), thyroid-related ophthalmopathy (13/171, 7.6%), infection, and inflammation. In tumors, metastatic tumor (n = 10) represented the most common subtype, followed by sarcoma (n = 9), retinoblastoma (n = 7), and lymphoma (n = 7). The four clinical cases aligned with these categories and illustrated a spectrum of outcomes—from irreversible vision loss in infection to visual preservation through timely endovascular intervention. This study provided a more detailed understanding of the diverse etiologies of acquired unilateral proptosis, suggesting the necessity of a multidisciplinary approach. Integrating these findings into clinical practice is expected to enhance early recognition, optimize treatment strategies, and ultimately improve patient outcomes.
Introduction
Proptosis, characterized as the forward displacement and protrusion of one or both eyes, can vary in duration and severity, with some cases resulting in visual impairment.[1] Proptosis can be classified as axial, when the underlying pathology is located within the extraocular muscle cone (intraconal), or nonaxial, when the abnormality is situated outside this region (extraconal).[2] Given its association with both vision-threatening and life-threatening conditions, prompt evaluation and appropriate management are essential. Although comprehensive global epidemiologic data on proptosis are limited—given that it is a presenting symptom rather than a singular diagnosis—existing studies indicate that it is among the most common initial signs of orbital pathology. In orbital tumor cohorts, proptosis has been reported as the predominant presenting feature, with its frequency ranging from 19.0 to 84.6%, depending on tumor type and study population.[3] In thyroid eye disease, the presence and severity of proptosis are closely correlated with disease progression.[4]
Accordingly, acquired unilateral proptosis presents a wide spectrum of etiologies, necessitating diverse treatment approaches based on the underlying cause. The four cases managed by the author also exhibited different etiologies of unilateral proptosis. In this study, these cases were presented alongside a literature review from the past 5 years, structured according to the classification proposed by Turnbull et al., which categorizes the causes into seven groups.[2] By providing a comprehensive overview, this study aimed to enhance awareness of etiological diversity of acquired unilateral proptosis, facilitating its application in clinical practice and underscoring its clinical significance.
Materials and Methods
Case Presentation
The following four cases of acquired unilateral proptosis encountered by the author were described. While proptosis improved with appropriate treatment, unfortunately, some cases resulted in complications such as permanent vision loss. The study was approved by the Institutional Review Board of our hospital (IRB number: 2019-07-018) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent for clinical photography was obtained from all patients.
-
A. Case 1: A 33-year-old female developed delayed intraorbital infection 6 years after craniofacial surgery for a traffic accident. She presented with progressive periorbital swelling and unilateral proptosis. Orbital computed tomography (CT) demonstrated +8.23 mm proptosis before treatment, related to severe maxillary sinusitis, and retained fixation implants. The presumed infection pathway was sinus–orbit communication along the implant surfaces. Despite multiple drainage procedures, implant removal, and prolonged systemic antibiotics, irreversible vision loss occurred. Follow-up CT confirmed resolution of proptosis (−0.27 mm) ([Fig. 1]).
-
B. Case 2: An 80-year-old male developed unilateral proptosis after a traffic collision causing a frontal cerebral hemorrhage and orbital roof fracture. Unilateral proptosis developed 5 days after the trauma, and CT showed +6.55 mm proptosis preoperatively. Intraoperatively, an intraorbital hematoma extending through the fractured orbital roof was identified. The patient underwent hematoma evacuation and orbital roof reconstruction, after which residual proptosis decreased to +1.03 mm on follow-up CT. Fortunately, visual acuity was fully preserved ([Fig. 2]).
-
C. Case 3: A 37-year-old male with LeFort I/II and sphenoidal sinus fractures developed unilateral proptosis 6 weeks after trauma. Initial CT demonstrated +10.92 mm proptosis. Cerebral angiography confirmed a carotid–cavernous fistula, and endovascular coiling was performed by neurosurgery. Posttreatment CT showed resolution of proptosis (−0.86 mm). His visual acuity was intact after treatment ([Fig. 3]).
-
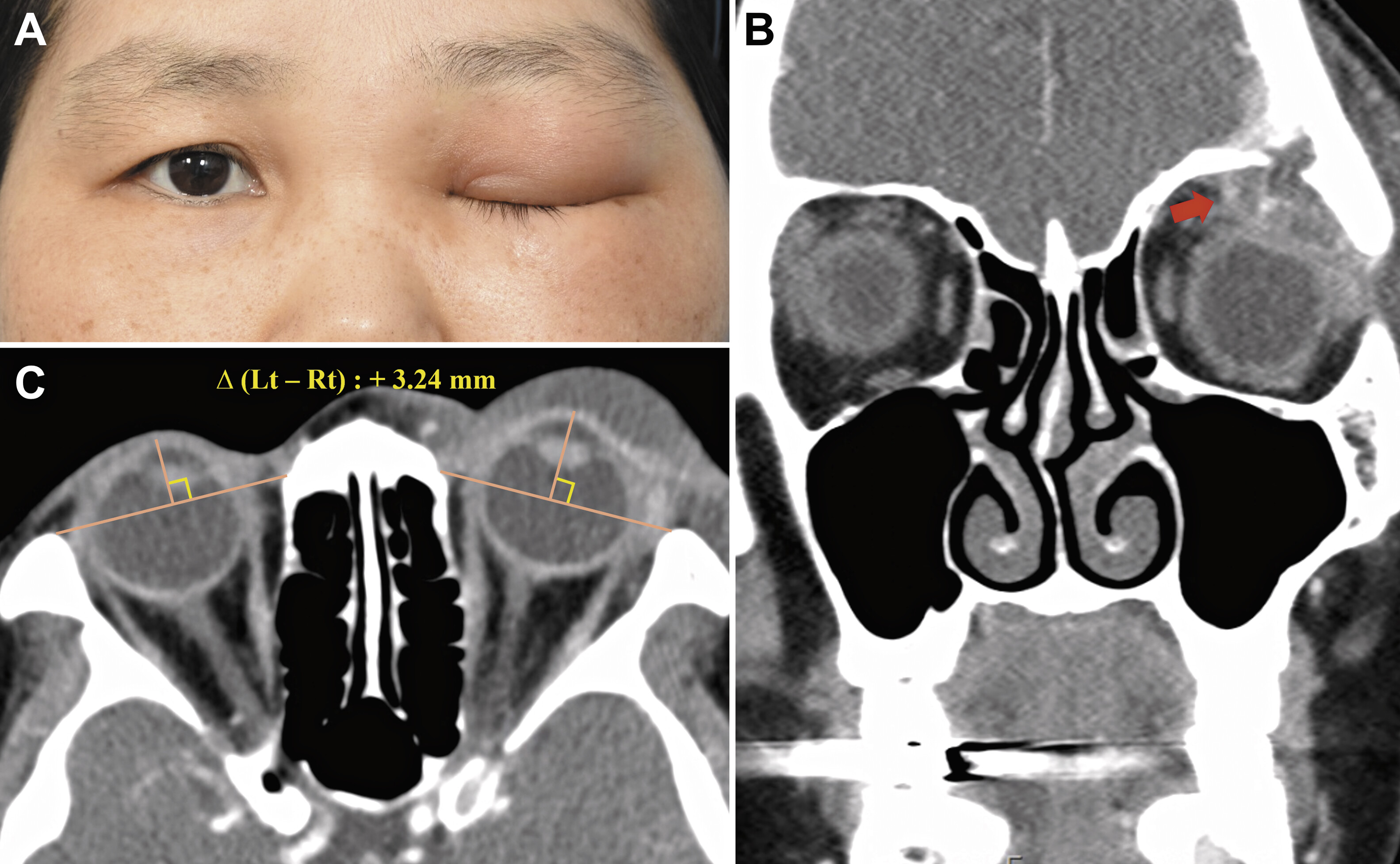
D. Case 4: A 41-year-old female with a history of breast cancer presented with unilateral proptosis. Orbital CT revealed +3.24 mm proptosis preoperatively, and intraoperative findings demonstrated an intraconal mass with orbital bony erosion. Histopathology confirmed metastatic carcinoma. The lesion was excised, but the patient was transferred for systemic oncological care and lost to follow-up. Vision was maintained until the last available examination ([Fig. 4]).



Literature Review
To achieve a comprehensive understanding of the etiologies of acquired unilateral proptosis, a systematic literature review was conducted using PubMed for articles published between January 1, 2020, and December 31, 2024. The search keyword was “(acquired OR unilateral) AND (exophthalmos OR proptosis),” yielding a total of 338 studies ([Fig. 5A]). Following a rigorous screening process, 164 studies were excluded due to irrelevant titles or abstracts, and an additional 3 records were removed due to retrieval or eligibility issues, resulting in 171 articles included for analysis[Supplementary Table 1]. Inclusion criteria were human studies reporting that acquired unilateral proptosis with an identifiable etiology, regardless of study type. Exclusion criteria were congenital or bilateral-only proptosis, editorials or letters without patient data, conference abstracts without sufficient data, and duplicate reports, for which the most complete version was retained. The study selection process was illustrated in [Fig. 5B], which follows the PRISMA 2020 flow diagram format.

Regardless of article type, each study was assessed based on its described etiology, with each reported cause counted as a single causative factor. The identified etiologies of proptosis were systematically classified into seven major categories:[2] thyroid-related, trauma, tumor, infection, inflammation, hemodynamic disorders, and miscellaneous causes.
Results
Among the seven etiological categories, tumors accounted for the largest proportion of acquired unilateral proptosis cases (93/171, 54.4%). A total of 30 different tumor types were identified, with metastatic tumors being the most common (n = 10), followed by sarcoma (n = 9), retinoblastoma (n = 7), and lymphoma (n = 7). Among infectious causes, fungal infections were the most frequently observed (n = 7). In the inflammatory category, which included six different conditions, idiopathic orbital inflammatory disease was the most prevalent, with 7 cases reported. Thyroid-related ophthalmopathy was reported in 13 cases. Interestingly, hemodynamic disorders represented the second most common etiology among the seven categories (24/171, 14.0%). A more detailed analysis revealed that orbital thrombosis (n = 8) was the most frequently reported vascular event, followed by carotid–cavernous fistula (n = 7; [Fig. 6]) To complement this etiological overview, a structured diagnostic algorithm was presented to assist clinical decision-making. The algorithm summarizes the typical diagnostic pathway, from radiological and laboratory evaluation to the major categories of differential diagnosis, and outlines representative treatment options for each ([Fig. 7]).


Discussion
The earliest reported case of acquired unilateral proptosis associated with the given keyword dates back to 1917, documenting a case of ethmoid osteoma.[5] Since then, numerous reports have described proptosis caused by thyroid-related conditions, tumors, and inflammatory diseases. However, due to the diagnostic limitations of imaging for intraconal lesions, early studies primarily focused on clinical symptoms and surgical exploration.[6] Efforts to develop noninvasive diagnostic methods for intraconal pathologies continued, and by the 1960s, contrast-enhanced X-ray and ultrasound were utilized to identify the underlying causes of proptosis.[7] [8] With the widespread adoption of CT and magnetic resonance imaging (MRI) in the 1970s and 1980s, nonsurgical diagnosis of intraconal lesions became significantly more accessible, leading to a substantial increase in research and clinical studies on proptosis. Accordingly, the diverse etiologies of acquired unilateral proptosis have become increasingly evident over the years.
Identifying the underlying etiology is essential, as treatment approaches vary significantly depending on the cause. Delayed diagnosis or inappropriate management may result in irreversible optic nerve damage and vision loss.[1] Therefore, when evaluating a patient with proptosis, clinicians must carefully consider how to rapidly and efficiently establish an accurate diagnosis to ensure prompt and appropriate intervention. The initial step in evaluating a patient with proptosis is a thorough physical examination. If the proptosis is pulsatile, potential causes to consider include congestive cardiac failure, aortic regurgitation, and arteriovenous malformations. In such cases, the CT angiography should be considered as a crucial diagnostic tool to rule out.[9] And, given the deep anatomical location of the orbit and surrounding structures, CT and MRI are generally recommended for diagnostic evaluation. CT imaging is particularly useful for detecting bony abnormalities and acute orbital compartment syndrome. A key radiologic finding to recognize is the “guitar pick sign,” which indicates acute increased intraocular pressure. This sign is characterized by a posterior globe angle of less than 120 degrees on CT, a finding that correlates with a poor prognosis and an increased risk of permanent vision loss.[10] When this occurs, immediate decompressive procedures such as lateral canthotomy should be performed. Additionally, MRI can provide superior visualization of intraorbital soft tissue injuries, including encephalocele and optic neuropathy. However, its limitations include longer scan times, reduced sensitivity to bony fragments and potential risks in patients with ferromagnetic foreign bodies.[10]
Thyroid function tests should not be overlooked in the diagnostic evaluation, as thyroid-related ophthalmopathy represents one of the leading causes of orbital inflammation. Its occurrence is estimated to range between 0.6 and 1.3 cases per 100,000 individuals annually.[11] While its exact pathophysiology remains unclear, proposed mechanisms include apical compression from enlarged extraocular muscles or fat, ischemia due to increased retrobulbar pressure, and perineural inflammation.[11] [12] Idiopathic orbital inflammation (IOI) is a benign, noninfectious, and nonspecific inflammatory condition of the orbit. It is the third most common orbital disease in adults, following thyroid-related ophthalmopathy and lymphoproliferative disorders.[13] Recent advancements in scientific research have led to increased investigation into the underlying pathogenesis of IOI. Two predominant theories have emerged: the autoimmune hypothesis and the viral infection hypothesis. While immune-mediated mechanisms have gained broader acceptance, a comprehensive and definitive pathophysiological explanation has yet to be established.[13]
In addition, in patients with a history of trauma or prior orbital surgery, potential complications such as delayed hemorrhage from implants or posttraumatic encephalocele could be considered.[9] [14] Notably, pediatric patients with orbital roof fractures demonstrating over 2-mm diastasis and associated frontal cerebral contusion may have an increased risk of developing intraorbital encephalocele.[15] Another uncommon but serious complication is orbital involvement following subgaleal hematoma. It results from blood accumulation under pressure at the superior orbital ridges, particularly in children, where the galea aponeurosis and periosteum attachments are loosely connected. The hematoma can dissect and detach the arcus marginalis from the orbital rim, leading to subperiosteal blood accumulation, which manifests as proptosis and decreased vision. Since coagulopathies can predispose patients to subgaleal hematoma, a thorough hematologic evaluation should be performed, including assessments of vitamin K levels, fibrinogen concentration, clotting factor deficiencies, and platelet disorders.[16]
Compared with previous articles, this review analysis underscores the predominance of tumors (54.4%) among acquired unilateral proptosis, while also quantifying other categories such as thyroid-associated disease, infection, trauma, and hemodynamic disorders. This highlights not only the relative frequency of major etiologies but also the diversity of underlying causes. The four representative cases serve as illustrative examples of the review findings. Case 1 demonstrated the vision-threatening course of orbital infection, echoing the poor visual outcomes described among infectious etiologies in the review. Case 2 illustrated traumatic orbital roof fracture with hematoma, reinforcing the importance of rapid intervention to preserve vision. Case 3 highlighted a hemodynamic disorder—carotid–cavernous fistula—emphasizing the critical role of timely endovascular intervention and interdisciplinary collaboration. Case 4 exemplified metastatic orbital disease, relating to the 10 metastatic tumors detected in the pooled analysis and reinforcing the need to consider systemic malignancy in new-onset unilateral proptosis. Collectively, these cases bridge the systematic data with real-world clinical practice, underscoring the necessity of tailored diagnostic and therapeutic approaches.
Conversely, very rare entities such as Erdheim–Chester disease,[17] hydatid disease,[18] or dengue-related orbital involvement,[19] while clinically intriguing, are worth acknowledging because they underscore the wide spectrum of potential etiologies. Even if their frequency is extremely low, awareness of such conditions may broaden the clinician's differential diagnosis and prevent overlooking rare but important causes of proptosis.
While our study incorporated the latest research, one limitation was the potential overrepresentation of rare case reports due to the nature of recently published literature. Additionally, diseases from original studies and case reports were counted equivalently, which may have introduced bias in the relative frequency of different etiologies. Moreover, this review relied primarily on PubMed, which provides comprehensive biomedical coverage; however, relevant articles indexed exclusively in other databases such as Embase or Scopus may not have been captured. Nevertheless, this study provided a more detailed understanding of the diverse etiologies of acquired unilateral proptosis, and these findings may indicate the need for a multidisciplinary approach involving plastic surgeons, ophthalmologists, radiologists, neurosurgeons, and endocrinologists for accurate diagnosis and effective management. Such collaboration is highly recommended, particularly in complex cases requiring comprehensive evaluation and coordinated treatment.
In conclusion, this study presented case reports of acquired unilateral proptosis and explored its diverse etiologies. Integrating these findings into clinical practice may help enhance early recognition, optimize treatment strategies, and ultimately improve patient outcomes.
Conflict of Interest
The authors declare that they have no conflict of interest.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Contributors' Statement
The author (N.-K.L.) performed all aspects of the study, including conceptualization, data collection, analysis, and manuscript writing.
Ethical Approval
The study was approved by the Institutional Review Board of our Hospital IRB number: 2019-07-018) and performed in accordance with the principles of the Declaration of Helsinki.
Informed Consent
All patients provided written informed consent for the publication and the use of their images.
-
References
- 1 Erickson BP, Johnson TEA. A 32-year-old man with delayed onset post-traumatic proptosis and diplopia. J Emerg Med 2014; 46 (04) 475-478
- 2 Turnbull A, Trikha S, Whaley C. et al. Acquired unilateral proptosis–an overview of aetiology and radiological considerations. RAD Magazine 2016; 42 (488) 15-17
- 3 Nathaniel GI, Eze UA, Onwuegbuna AA, Echieh CI, Alen HA. Pattern of orbito-ocular tumours in Nigeria: a systematic review. BMC Cancer 2025; 25 (01) 224
- 4 Tamhankar MA, Raza S, Brutsaert E. et al. The burden of illness in thyroid eye disease: current state of the evidence. Front Ophthalmol (Lausanne) 2025; 5 (05) 1565762
- 5 Sattler R. A case of unilateral proptosis. exploratory operation. tentative diagnosis of an ethmoid osteoma. Trans Am Ophthalmol Soc 1917; 15: 238-242
- 6 Naffziger HC. Progressive exophthalmos. Ann R Coll Surg Engl 1954; 15 (01) 1-24
- 7 Lee MJ, Verma R, Hamilton BE. et al. The utility of orbital imaging in the evaluation of orbital disease. PLoS One 2024; 19 (08) e0308528
- 8 Nagaraj UD, Koch BL. Imaging of orbital infectious and inflammatory disease in children. Pediatr Radiol 2021; 51 (07) 1149-1161
- 9 Ha AY, Mangham W, Frommer SA. et al. Interdisciplinary management of minimally displaced orbital roof fractures: delayed pulsatile exophthalmos and orbital encephalocele. Craniomaxillofac Trauma Reconstr 2017; 10 (01) 11-15
- 10 Mungroo KA, Song A, Greenstein J, Hahn B. Man with proptosis. Ann Emerg Med 2023; 82 (04) 438-448
- 11 Iao TWU, Rong SS, Ling AN, Brelén ME, Young AL, Chong KKL. Electrophysiological studies in thyroid associated orbitopathy: a systematic review. Sci Rep 2017; 7 (01) 12108
- 12 Panagiotou G, Perros P. Asymmetric graves' orbitopathy. Front Endocrinol (Lausanne) 2020; 11: 611845
- 13 Fang Y, Shen B, Dai Q, Xie Q, Wu W, Wang M. Orbital inflammatory pseudotumor: new advances in diagnosis, pathogenesis, and treatment. Eur J Med Res 2023; 28 (01) 395
- 14 Ryu YA, Park JB, Kyung HW, Song SH, Kang NH. Delayed orbital hemorrhage around alloplastic implants after blowout fracture reduction. Arch Craniofac Surg 2015; 16 (01) 35-38
- 15 Satyarthee GD, Kumar A. Posttraumatic giant fronto-orbito encephalocele causing cosmetic disfiguring forehead swelling with proptosis: Management. J Pediatr Neurosci 2016; 11 (04) 341-343
- 16 Jenkins TL, Zheng CX, Murchison AP, Bilyk JR. Orbital compartment syndrome following post-traumatic subgaleal hematoma. Ophthalmic Plast Reconstr Surg 2017; 33 (02) e33-e36
- 17 Merritt H, Pfeiffer ML, Richani K, Phillips ME. Erdheim-Chester disease with orbital involvement: case report and ophthalmic literature review. Orbit 2016; 35 (04) 221-226
- 18 Thapa S, Ghosh A, Ghartimagar D, Shrestha S, Lalchan S, Talwar OP. Hydatidosis of infratemporal fossa with proptosis - an unusual presentation: a case report and review of the literature. J Med Case Rep 2018; 12 (01) 309
- 19 Maan V, Guha S, Sapra H, Chauhan L. Ocular and adnexal manifestations post dengue hemorrhagic fever. Indian J Ophthalmol 2024; 72 (10) 1495-1500
Correspondence
Publication History
Received: 30 April 2025
Accepted: 06 October 2025
Article published online:
22 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Erickson BP, Johnson TEA. A 32-year-old man with delayed onset post-traumatic proptosis and diplopia. J Emerg Med 2014; 46 (04) 475-478
- 2 Turnbull A, Trikha S, Whaley C. et al. Acquired unilateral proptosis–an overview of aetiology and radiological considerations. RAD Magazine 2016; 42 (488) 15-17
- 3 Nathaniel GI, Eze UA, Onwuegbuna AA, Echieh CI, Alen HA. Pattern of orbito-ocular tumours in Nigeria: a systematic review. BMC Cancer 2025; 25 (01) 224
- 4 Tamhankar MA, Raza S, Brutsaert E. et al. The burden of illness in thyroid eye disease: current state of the evidence. Front Ophthalmol (Lausanne) 2025; 5 (05) 1565762
- 5 Sattler R. A case of unilateral proptosis. exploratory operation. tentative diagnosis of an ethmoid osteoma. Trans Am Ophthalmol Soc 1917; 15: 238-242
- 6 Naffziger HC. Progressive exophthalmos. Ann R Coll Surg Engl 1954; 15 (01) 1-24
- 7 Lee MJ, Verma R, Hamilton BE. et al. The utility of orbital imaging in the evaluation of orbital disease. PLoS One 2024; 19 (08) e0308528
- 8 Nagaraj UD, Koch BL. Imaging of orbital infectious and inflammatory disease in children. Pediatr Radiol 2021; 51 (07) 1149-1161
- 9 Ha AY, Mangham W, Frommer SA. et al. Interdisciplinary management of minimally displaced orbital roof fractures: delayed pulsatile exophthalmos and orbital encephalocele. Craniomaxillofac Trauma Reconstr 2017; 10 (01) 11-15
- 10 Mungroo KA, Song A, Greenstein J, Hahn B. Man with proptosis. Ann Emerg Med 2023; 82 (04) 438-448
- 11 Iao TWU, Rong SS, Ling AN, Brelén ME, Young AL, Chong KKL. Electrophysiological studies in thyroid associated orbitopathy: a systematic review. Sci Rep 2017; 7 (01) 12108
- 12 Panagiotou G, Perros P. Asymmetric graves' orbitopathy. Front Endocrinol (Lausanne) 2020; 11: 611845
- 13 Fang Y, Shen B, Dai Q, Xie Q, Wu W, Wang M. Orbital inflammatory pseudotumor: new advances in diagnosis, pathogenesis, and treatment. Eur J Med Res 2023; 28 (01) 395
- 14 Ryu YA, Park JB, Kyung HW, Song SH, Kang NH. Delayed orbital hemorrhage around alloplastic implants after blowout fracture reduction. Arch Craniofac Surg 2015; 16 (01) 35-38
- 15 Satyarthee GD, Kumar A. Posttraumatic giant fronto-orbito encephalocele causing cosmetic disfiguring forehead swelling with proptosis: Management. J Pediatr Neurosci 2016; 11 (04) 341-343
- 16 Jenkins TL, Zheng CX, Murchison AP, Bilyk JR. Orbital compartment syndrome following post-traumatic subgaleal hematoma. Ophthalmic Plast Reconstr Surg 2017; 33 (02) e33-e36
- 17 Merritt H, Pfeiffer ML, Richani K, Phillips ME. Erdheim-Chester disease with orbital involvement: case report and ophthalmic literature review. Orbit 2016; 35 (04) 221-226
- 18 Thapa S, Ghosh A, Ghartimagar D, Shrestha S, Lalchan S, Talwar OP. Hydatidosis of infratemporal fossa with proptosis - an unusual presentation: a case report and review of the literature. J Med Case Rep 2018; 12 (01) 309
- 19 Maan V, Guha S, Sapra H, Chauhan L. Ocular and adnexal manifestations post dengue hemorrhagic fever. Indian J Ophthalmol 2024; 72 (10) 1495-1500