

Subscribe to RSS
DOI: 10.1055/a-2565-9342
Novel Strategies for Expanding the Endoscopic Caudal Access to the Craniovertebral Junction: A Cadaveric Comparative Analysis of Nasofrontal Trephination and Posterior Palatectomy
Authors
Financial Support There was no financial or funding support for the project.

Abstract
Objectives
Although the endoscopic endonasal approach (EEA) has emerged as a preferred alternative to traditional transoral access for craniovertebral junction (CVJ) surgery, its limited inferior reach beyond the C1 level remains a significant challenge. This study investigates the effectiveness of using a contralateral nasofrontal trephination (CNT) or a posterior palatectomy (PP) to enhance the caudal reach to the CVJ region.
Design
A quantitative cadaveric study.
Setting
Cadaver dissection laboratory.
Participants
A total of 15 adult human cadaveric heads.
Methods
EEA, EEA + PP, and EEA + CNT approaches to the CVJ were performed. Neuronavigation was used for objective measurements quantifying the volume of surgical freedom, surface area of deep exposure, entry point sagittal angle, and inferior reach below the odontoid process.
Main Outcome Measures and Results
EEA + CNT demonstrated superior surgical metrics across all parameters. Surface exposure was significantly greater with EEA + CNT (107.04 cm2) versus EEA + PP (86.26 cm2) and standard EEA (69.78 cm2; p < 0.001). The volume of surgical freedom showed similar superiority with EEA + CNT (60.21 cm3), followed by EEA + PP (34.14 cm3) and EEA (26.13 cm3; p < 0.001). Inferior reach below the odontoid (CNT: 6.35 cm; PP: 2.17 cm; EEA: 0.9 cm; p < 0.0001) and surgical trajectory angle (CNT: 50.1 degrees; PP: 21.4 degrees; EEA: 16.6 degrees; p < 0.0001) demonstrated significant stepwise improvements with each adjunct technique.
Conclusion
Both CNT and PP techniques significantly enhance the surgical corridor of traditional EEA for CVJ access. A CNT afforded superior surgical exposure while maintaining minimal invasiveness. PP offers a viable alternative when external incisions are undesired and lesions are confined within the C2–C3 level.
Keywords
3D photogrammetry - craniovertebral junction - endoscopic endonasal approach - endoscopic endonasal odontoidectomy - multiport endoscopic surgery - nasofrontal trephination - posterior palatectomy - quantitative analysis - skull baseIntroduction
The transoral trans-pharyngeal approach was historically the mainstay method of accessing the craniovertebral junction (CVJ) in patients with basilar invagination, odontoid fractures, or tumors.[1] However, this technique has drawbacks, presenting an increased risk of aerodigestive tract morbidities, such as postoperative dysphagia associated with nasal regurgitation and aspiration and the need for prolonged nasogastric tube feeding and edema with airway obstruction, all leading to an extended recovery period.[2] [3] Recently, the endoscopic endonasal approach (EEA) has emerged as a minimally invasive alternative for odontoidectomy and anterior decompression of the CVJ. Others have shown that EEA is associated with lower rates of postoperative dysphagia and respiratory complications.[4] [5] The neurologic and quality of life (QOL) outcomes following EEA are equal to those seen with traditional transoral approaches.[6] [7] Also, nasal-specific QOL does not appear adversely affected by EEA.[8] However, the EEA has a higher incidence of cerebrospinal fluid (CSF) leaks, both intraoperative (30%) and postoperative (5.2%), compared with the transoral approach.[9] Conversely, advancements in surgical techniques, including multilayered reconstructions and the application of vascularized flaps, have significantly reduced the incidence of postoperative CSF leaks. These developments have rendered the potential for a CSF leak a minor consideration in the selection of a surgical approach for the CVJ. Additionally, the panoramic view provided by the endoscope allows for superior visualization and detailed dissection, improving the precision and safety of the procedure.[10] Therefore, the remaining primary challenge in endoscopic odontoidectomy and ventral decompression of the CVJ lies in the anatomical constraints of the endonasal corridor. The exposure of the approach to the CVJ is restricted caudally by the hard palate and laterally by the tori and eustachian tubes.[11] These anatomical constraints underscore the need for modifications to enhance the caudal exposure without compromising the minimally invasive nature of the technique. This study introduces two innovative techniques, the contralateral nasofrontal trephination (CNT) and posterior palatectomy (PP), designed to overcome the constraints of the EEA in addressing challenges such as limited surgical exposure, difficulty in dural reconstruction, and reduced inferior reach during endonasal odontoidectomy and minimally invasive CVJ surgery. The study evaluates the anatomical access achieved with these techniques, comparing the limitations of exposure instrumentation of a standard EEA to those of an EEA combined with a CNT or a PP.
Materials and Methods
An endoscopic endonasal approach to the CVJ was performed on 15 adult human cadaveric specimens at the Anatomy Laboratory Toward Visuospatial Surgical Innovations in Otolaryngology and Neurosurgery (ALT-VISION) of the Wexner Medical Center of The Ohio State University. ALT-VISION and all researchers comply with university and government regulations regarding the use of human tissues. All specimens had been previously prepared, isolating the common carotid and vertebral arteries to cannulate and flush with warm water, thus clearing blood clots over three sessions. Subsequently, the vessels were injected with red and blue latex dye for the arterial and venous systems, respectively, to better visualize them during the dissections. All specimens were kept in a 70% alcohol solution throughout the procedure.
Visualization was provided with 0-degree and 30-degree rod-lens endoscopes of 4 mm diameter and 18 cm length (Karl Storz Endoscopy; Karl Storz, Tuttlingen, Germany) paired with a high-definition camera and video monitor. Video and digital images of the dissections were recorded during dissections using the AIDA recording system (Karl Storz Endoscopy; Karl Storz, Tuttlingen, Germany). Following the placement of five screws spanning the entire cranium, the specimens were scanned with a high-resolution multiplanar 1-mm cut computed tomography (CT). Standard endonasal instruments, along with a high-speed drill (Medtronic Corp; Jacksonville, FL), were used for the dissection. Digital Imaging and Communication in Medicine (DICOM) data were exported to a neuronavigation software (v. 1, GTx-Eyes II Approach Viewer, University Health Network, University of Toronto, Toronto, ON, Canada) to visualize the measurements of the endoscopic corridors recorded during the dissections, according to the validated method previously described by our group for the quantifications of various surgical approaches.[12] [13] [14] Quantitative radiological and anatomical measurements were performed based on the cadaveric surgical dissections.
Contralateral Nasofrontal Trephination (CNT) Approach
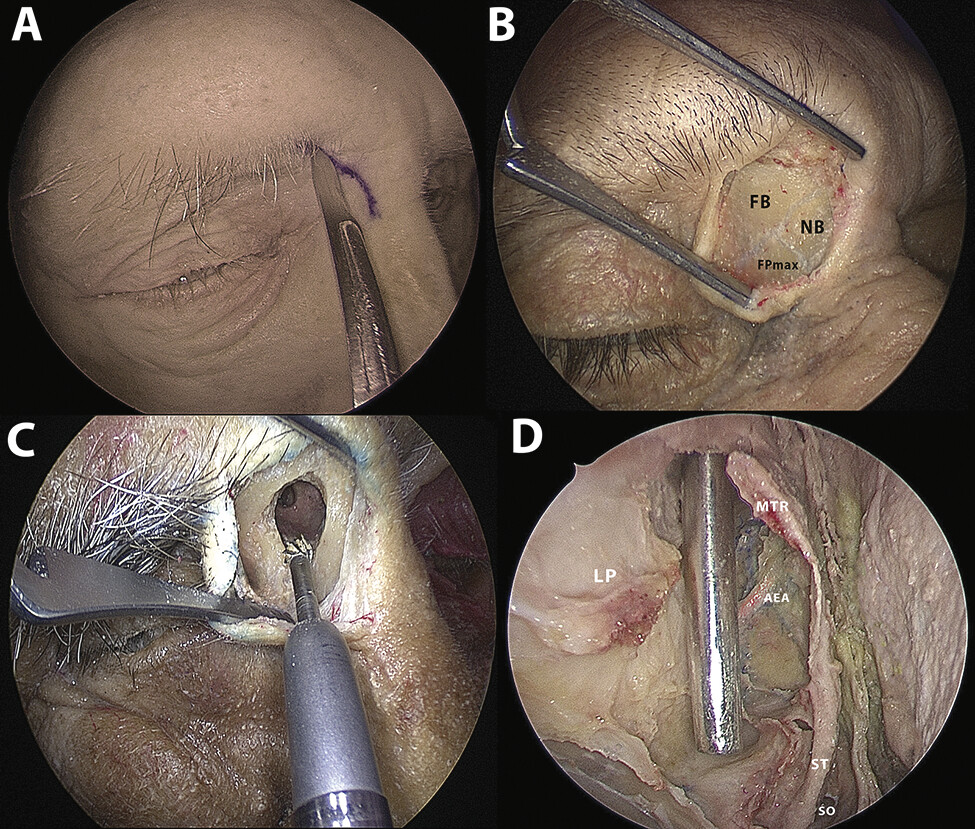
A 1.5-cm nasofrontal incision was performed between the nasal dorsum and the medial end of the eyebrow. The incision was carried down to bone, and the periosteum was elevated to reveal the meeting point between two suture lines separating three bones: the glabella of the frontal bone, the nasal bone, and the frontal process of the maxillary bone. Then, a trephine of 1.5 cm × 1.0 cm was drilled at this intersection, opening into the frontal recess ([Fig. 1]), following an inferomedial trajectory to avoid skull base injury as described. An inferomedial trajectory of the drill tip was confirmed to avoid injuring the skull base[15] ([Fig. 2]). A three-dimensional photogrammetry-generated model was rendered using RealityCapture software 1.5 (Epic Games) to illustrate the CNT approach trajectory toward the CVJ region (3D Model 1; https://sketchfab.com/3d-models/cnt-approach-corridor-to-cvj-018a2df55bbe426094511beb6974a5f8).

3D Model 1 The nasofrontal trephination and the trajectory of a dissector introduced through the contralateral nasofrontal trephination (CNT) port and directed toward the craniovertebral junction (CVJ). https://sketchfab.com/3d-models/cnt-approach-corridor-to-cvj-018a2df55bbe426094511beb6974a5f8.
Endonasal Corridor
An EEA was performed by out-fracturing inferior turbinates, followed by anterior and posterior ethmoidectomies ipsilateral to the trephination. Anatomical landmarks around the CNT entry corridor were identified, including the anterior ethmoidal artery, the lamina papyracea, and the middle turbinate. A Draf II B procedure was then completed to enhance maneuverability and surgical freedom through the frontal recess (a Draf II A was sufficient to allow instrument access). This was followed by a posterior septectomy and removal of the sphenoid rostrum. The floor of the sphenoid sinus was drilled posteriorly to be flush with the clival recess, and anatomical landmarks, including foramina lacera, fossae of Rosenmüller, and eustachian tubes tori, were identified and preserved to serve as the lateral limits of the initial dissection.
Dissection of the Lower Clivus and the Craniovertebral Junction
The nasopharyngeal mucosa was incised in an inverted-U shape and reflected inferiorly, extending from the level of the sphenoid sinus floor down to the level of the soft palate. This allowed the exposure of the underlying pharyngobasilar fascia and the median raphe covering the prevertebral muscles. After the removal of the prevertebral fascia, the recti capitis anterior muscles were dissected, and the longi capitis muscles were lateralized. The anterior longitudinal ligament was exposed and dissected, revealing the underlying anterior atlantooccipital membrane. Key anatomical structures, including the foramen magnum arch, pharyngeal tubercle, occipital condyles, supracondylar grooves, and C1 vertebral arch, were exposed. The odontoid process was exposed with the attached apical and alar ligaments. Using the CNT, the odontoid process was drilled with the preservation of the C1 vertebral arch ([Fig. 3]). The most cranial portion of the odontoid process is identified behind the anterior arch of the atlas. Endoscopic visualization and instrumentation comparisons were made toward the C2, C3, and C4 vertebrae ([Fig. 4]). A three-dimensional photogrammetry-generated model was rendered using RealityCapture software 1.5 (Epic Games), showing the surgical dissection and visualization of the CVJ region using combined EEA and CNT approaches (3D Model 2; https://sketchfab.com/3d-models/craniovertebral-junction-reach-from-cnt-approach-472c78ee221b40539c51ffa64b836df0).


3D Model 2 Surgical dissection and visualization of the craniovertebral junction (CVJ) region using combined endoscopic endonasal approach (EEA) and contralateral nasofrontal trephination (CNT) approaches with maximum inferior reach till the C4 vertebra. https://sketchfab.com/3d-models/craniovertebral-junction-reach-from-cnt-approach-472c78ee221b40539c51ffa64b836df0.
Posterior Palatectomy (PP) Approach
This technique began with the elevation of a posteriorly based nasal floor mucosal flap, which involves three incisions, one horizontal incision at the level of the transverse palatine suture near the conchal crest and two vertical incisions separating the flap from the lateral nasal wall and septal mucosa. The flap was then reflected posteriorly, exposing the transverse palatine suture between the horizontal plate of the palatine bone posteriorly and the palatine process of the maxillary bone anteriorly ([Fig. 5A]).

Subsequently, the horizontal plate of the palatine bone was carefully thinned using a high-speed drill until a delicate bony shell remained. This created a quadrangular bony window, leaving approximately half a centimeter of bone intact on both sides and continuous with the lateral nasal wall to safeguard the greater and lesser palatine foramina along with their associated artery and nerve. The thin bony shell was subsequently removed, including the posterior nasal spine, while preserving the underlying periosteum and palatal muscles. This technique allowed for preserving the underlying periosteum and palatal muscles. The mucosal floor flap could then be repositioned seamlessly ([Fig. 5]; [Video 1]). A three-dimensional photogrammetry-generated model was rendered using RealityCapture software 1.5 (Epic Games), illustrating the PP approach and the quadrangular bony window created (3D Model 3; https://sketchfab.com/3d-models/cvj-view-posterior-palatectomy-218a60bad54643e999ea51241908269a).
Video 1 This video describes the contralateral nasofrontal trephination, and the posterior palatectomy techniques as two promising approaches to expand the access to the craniovertebral junction inferiorly.3D Model 3 The craniovertebral junction (CVJ) region dissection after the posterior palatectomy approach, illustrating the quadrangular bony window created within the horizontal plate of the palatine bone. https://sketchfab.com/3d-models/cvj-view-posterior-palatectomy-218a60bad54643e999ea51241908269a.
The EEA was performed first, followed by CNT, with the PP conducted last to avoid potential measurement bias associated with palate drilling.
Quantitative Analysis
The following parameters were studied for the EEA-only, and for the PP and CNT as complementary approaches to the EEA.
(1) Area of surface exposure and volume of surgical freedom: Studied on 10 cadavers.
Rendering of the target area was obtained from the CT scans of all specimens using ITK-SNAP software (v. 4.0.2). The study focused on the paramedian region, delimited superiorly by an axial plane passing at the level of the superior border of the C1 arch, while inferiorly the limit was represented by an axial plane at the level of the inferior margin of C4. The lateral borders were limited by a sagittal plane that passed through the most medial limit of the lateral masses of the first cervical vertebrae. Therefore, four different regions were identified, defined as the anterior surface of C1, the anterior surface of C2, the anterior surface of C3, and the anterior surface of C4. Contouring the desired region in each consecutive CT axial slice, each surgical volume was intersected with the target areas drawn in GTx-Eyes II Approach Viewer to obtain the value ([Fig. 6A]).

The volume of surgical freedom was defined as the maximal available working volume with respect to a specific surgical corridor and target structure. The key structures comprised four midline points from superior to inferior: the odontoid process, C1 arch, body of C2, body of C3, and body of C4 vertebrae, respectively. To achieve this, GTx-Eyes II Approach Viewer (v. 1, GTx-Eyes II Approach Viewer, University Health Network, University of Toronto, Toronto, ON, Canada) was used to visualize volumes and deep areas of each approach as a surgical truncated pyramid, as previously defined by Andaluz et al.[16] The truncated pyramid was based at the nose for the EEA and EEA + PP and at the frontal trephination window for EEA + CNT ([Fig. 6B–D]).
(2) Reach and angles around the CVJ: Measured on 15 cadavers using the image guidance system.
The distance reached below the odontoid for each approach was calculated ([Fig. 7A]), and the angles around the CVJ related to the entry point of each approach were measured, including:
-
The naso-palatine angle, which was taken as a reference sagittal angle for the EEA, was defined as the angle between the defined nasoaxial line[17] and the hard palate line meeting at the posterior nasal spine point ([Fig. 7B]).
-
The naso-maxillary angle, which was taken as a reference sagittal angle for the EEA + PP approach, was defined as the angle between the nasoaxial line and the hard palate line meeting at the level of the transverse palatine suture ([Fig. 7C]).
-
The fronto-palatine angle, which was taken as a reference sagittal angle for the CNT, was defined as the angle between the trajectory of a line drawn from the CNT entry and the hard palate line (fronto-palatine line) meeting at the posterior nasal spine ([Fig. 7D]).

Statistical Analysis
The distribution of continuous variables (volume of surgical freedom, surface area, entry point angle, and distance below odontoid) was represented using boxplots. The Shapiro-Wilk test was used to assess data normality distribution, and Levene's test was applied to confirm the homogeneity of variances. One-way analysis of variance (ANOVA) was performed to compare the means between the three surgical approaches (EEA, EEA + PP, and EEA + CNT), followed by Tukey's HSD (honestly significant difference) post hoc analysis for multiple comparisons. All statistical analyses were performed using JASP statistical software (Version 0.19.1.0).
Results
Area of Exposure
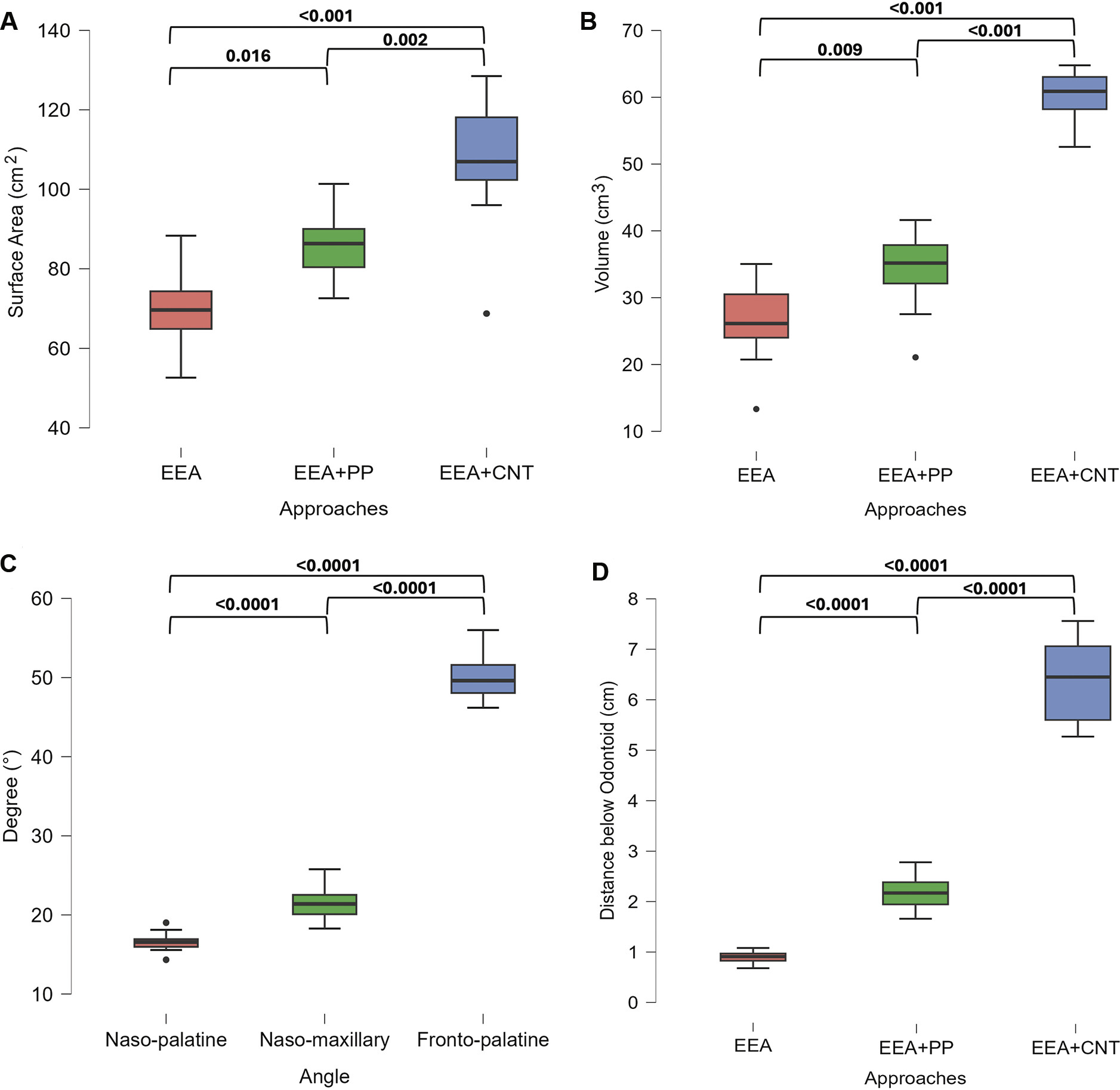
The mean areas of surface exposure were 69.78 ± 9.87 cm2 (EEA), 86.26 ± 8.40 cm2 (EEA + PP), and 107.04 ± 17.07 cm2 (EEA + CNT). A one-way ANOVA was conducted to compare the effects of the three approaches (EEA, EEA + PP, and EEA + CNT) on the surface area. ANOVA revealed significant differences among the approaches (p < 0.001), and Tukey's HSD post-hoc comparisons revealed significant differences between EEA and EEA + CNT (p < 0.001), EEA + PP and EEA + CNT (p = 0.002), and EEA and EEA + PP (p = 0.016) ([Fig. 8A]).
Volume of Surgical Freedom
For the volume of surgical freedom, the means were 26.13 ± 6.19 cm3 for EEA, 34.14 ± 6.23 cm3 for EEA + PP, and 60.21 ± 3.82 cm3 for EEA + CNT with significant differences among groups (p < 0.001) confirmed by ANOVA. Tukey's HSD post-hoc analysis comparisons showed significant differences for pairwise comparisons between EEA and EEA + CNT (p < 0.001), EEA + PP and EEA + CNT (p < 0.001), and EEA and EEA + PP (p = 0.009) ([Fig. 8B]).
Entry Point Angle
The entry point angles averaged 16.6 ± 1.13 degrees for naso-palatine, 21.4 ± 2.01 degrees for naso-maxillary, and 50.1 ± 3.10 degrees for fronto-palatine approaches with post-hoc comparisons showing significant differences among and between all groups (p < 0.0001) ([Fig. 8C]).
Reach Below the Odontoid Process
The mean distances reached below the odontoid process were 0.9 ± 0.11 cm (EEA), 2.17 ± 0.3 cm (PP), and 6.35 ± 0.8 cm (CNT). Post-hoc analysis revealed significant differences between all the approaches (p < 0.0001) ([Fig. 8D]).
Discussion
Anterior approaches for decompressing the CVJ can be broadly classified into three main techniques: transoral, transcervical, and transnasal.[6] Historically, the transoral and transcervical routes implied an open surgical procedure with direct visualization; however, modern advancements now incorporate endoscopic assistance to improve outcomes.[18] [19] [20] We propose that the endonasal approach offers untapped potential for further development of CVJ surgery, historically considered a “no man's land.”
Current literature demonstrates that although both transoral and transnasal approaches provide adequate exposure at the C1 level, the endonasal approach is less effective in lower regions.[21] The feasibility of a transnasal endoscopic odontoidectomy relies on the preoperative assessment of the radiological “nasoaxial line” to gauge the maximal inferior extent of the surgical corridor.[17] However, recent studies doubt these predictive measures and suggest that hard palate length is the only reliable predictor.[22] To overcome the lower reach limitation, we evaluated two novel adjunct approaches innovated by our research group: the CNT and the PP.[15] [23] The nasofrontal trephination was preferred to be performed on the contralateral side of the long axis of the lesion, as this will provide the most direct visualization and instrumentation. Overall, the two techniques added to the caudal exposure and reach of the core endonasal surgical corridor.[24] [25] [26]
In this study, the standard EEA exposure extended to the C1–C2 junction level, which is consistent with the literature.[21] In comparison, the CNT approach extended the caudal reach to the upper half of the C4 vertebra, while a PP extended the caudal reach to the C2–C3 junction, both surpassing the nasoaxial line limitation. Quantitatively, the mean distance reached below the odontoid for both the CNT and the PP was statistically significant compared with the EEA alone (p < 0.0001). Reaching these more caudal levels may allow access to pathologies located at or below the C2 level, which can be critical for adequate decompression in select patients, particularly for treating conditions such as basilar invagination, rheumatoid pannus, and neoplasms that involve the lower CVJ and upper cervical spine.
The CNT approach offers several distinct advantages. First, it enables complete access to the odontoid process till its base while preserving the C1 arch and the transverse ligament of the atlas through straight instrumentation. This preservation of atlantoaxial joint stability may potentially eliminate the need for postoperative cervical spine fixation. However, this requires further research and clinical correlation.[27] Additionally, the CNT approach offers excellent postoperative cosmetic outcomes, as its incision can be discreetly hidden within the medial part of the eyebrow.[28] [29] Although curved instruments can enhance the inferior reach of EEA, similar benefits apply to the PP and CNT approaches, albeit with inherent limitations such as reduced maneuverability and blind spots around the instrument tip. Furthermore, in cases of extensive lesions with lateral extension, particularly those extending to the infrapetrous region, the CNT's superior sagittal angle of attack, resulting from its higher entry point, eliminates the need for eustachian tube mobilization by providing direct access behind it, ensuring an unobstructed surgical corridor.[30] The approach's entry point at the frontal recess provides an additional safety advantage, positioning below the skull base and avoiding olfactory fiber injury. The enhanced fronto-palatine angle achieved with a CNT offers superior directional access to the CVJ compared with standard EEA and EEA + PP. This steeper trajectory allows for improved visualization and instrumentation.[17]
The area of deep exposure reflects the accessible surgical surface centered on the target anatomy, while the volume of surgical freedom represents the maneuverability within the corridor for optimal use of surgical instruments and effective visualization. Both CNT and PP techniques demonstrated significant improvements in the area of deep exposure and volume of surgical freedom compared with the standard EEA, with the CNT showing particular advantages for extensive surgical manipulation.
This improvement reduces instrument conflict by creating a new ergonomic axis and, thus, may be clinically significant. A notable innovation of the CNT is its creation of a secondary instrumentation axis, effectively minimizing instrument conflict “fencing effect,” where instruments conflict within a single axis, through a dual-port configuration. This setup enables simultaneous operation by multiple surgeons, potentially enhancing procedural efficiency.[31] [32] [33] Additionally, we were able to introduce two instruments through the CNT port. However, the trade-off involved some reduction in maneuverability due to the rigid bony boundaries of the access port. Future studies should explore refining nasofrontal trephination ergonomics to optimize instrument flexibility without compromising the benefits of expanded access. Our cadaveric experience suggests that the CNT approach is particularly advantageous for lesions with significant caudal extensions, while the PP presents a viable alternative for lesions confined within the C2–C3 caudal limit, especially in cases where CNT may be less feasible or when additional external incisions are undesirable.
Regarding the PP technique, the maximum safe drilling window was achieved by targeting the horizontal plate of the palatine bone. However, removing only the posterior nasal spine and a small surrounding segment of bone can also effectively enhance paramedian inferior access to the CVJ. It is important to note that only the bony component should be removed while preserving the underlying periosteum, as overly aggressive resection may lead to complications such as velopharyngeal insufficiency with voice changes and nasal regurgitation or the development of a palatal fistula. The lateral extension of palatine bone drilling was performed to improve surgical maneuverability and to demonstrate the maximum bone removal possible when addressing lesions that extend more laterally. Also, the PP, which includes raising the posteriorly based nasal floor mucosal flap,[34] maintains the traditional endonasal axis while modestly improving surgical exposure.
Conclusion
This study highlights the advantages of the CNT and PP approaches as adjuncts to the EEA for CVJ access. Both the techniques contributed to the caudal exposure and instrument reach of a basic EEA to the CVJ. The CNT approach offered the widest exposure, largest surgical freedom, and best caudal reach. These findings suggest that incorporating CNT or PP can expand the EEA's versatility, potentially improving outcomes for CVJ pathologies. Further clinical validation is needed to confirm these benefits. This cadaveric study carries some implied limitations as the observed tissue pliability may not fully replicate what occurs in living patients, and the absence of pathological lesions limits the ability to model the anatomic distortions that may arise in clinical scenarios.
Conflict of Interest
None declared.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
This article was selected to receive the Rhoton Award at the 34th North American Skull Base Society Conference in New Orleans, Louisiana, USA, 2025.
-
References
- 1 Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R. The expanded endonasal approach: a fully endoscopic transnasal approach and resection of the odontoid process: technical case report. Neurosurgery 2005; 57 (1, Suppl): E213 , discussion E213
- 2 Ponce-Gómez JA, Ortega-Porcayo LA, Soriano-Barón HE. et al. Evolution from microscopic transoral to endoscopic endonasal odontoidectomy. Neurosurg Focus 2014; 37 (04) E15
- 3 Visocchi M, Signorelli F, Liao C. et al. Transoral versus transnasal approach for craniovertebral junction pathologies: never say never. World Neurosurg 2018; 110: 592-603
- 4 Halderman AA, Barnett SL. Endoscopic endonasal approach to the craniovertebral junction. World J Otorhinolaryngol Head Neck Surg 2022; 8 (01) 16-24
- 5 Morales-Valero SF, Serchi E, Zoli M, Mazzatenta D, Van Gompel JJ. Endoscopic endonasal approach for craniovertebral junction pathology: a review of the literature. Neurosurg Focus 2015; 38 (04) E15
- 6 Fang CH, Friedman R, Schild SD. et al. Purely endoscopic endonasal surgery of the craniovertebral junction: a systematic review. Int Forum Allergy Rhinol 2015; 5 (08) 754-760
- 7 Gempt J, Lehmberg J, Grams AE, Berends L, Meyer B, Stoffel M. Endoscopic transnasal resection of the odontoid: case series and clinical course. Eur Spine J 2011; 20 (04) 661-666
- 8 Ottenhausen M, Alalade AF, Rumalla K. et al. Quality of life after combined endonasal endoscopic odontoidectomy and posterior suboccipital decompression and fusion. World Neurosurg 2018; 116: e571-e576
- 9 Shriver MF, Kshettry VR, Sindwani R, Woodard T, Benzel EC, Recinos PF. Transoral and transnasal odontoidectomy complications: a systematic review and meta-analysis. Clin Neurol Neurosurg 2016; 148: 121-129
- 10 Fujii T, Platt A, Zada G. Endoscopic endonasal approaches to the craniovertebral junction: a systematic review of the literature. J Neurol Surg B Skull Base 2015; 76 (06) 480-488
- 11 Joaquim AF, Osorio JA, Riew KD. Transoral and endoscopic endonasal odontoidectomies—surgical techniques, indications, and complications. Neurospine 2019; 16 (03) 462-469
- 12 Doglietto F, Qiu J, Ravichandiran M. et al. Quantitative comparison of cranial approaches in the anatomy laboratory: a neuronavigation based research method. World J Methodol 2017; 7 (04) 139-147
- 13 Doglietto F, Radovanovic I, Ravichandiran M. et al. Quantification and comparison of neurosurgical approaches in the preclinical setting: literature review. Neurosurg Rev 2016; 39 (03) 357-368
- 14 Doglietto F, Ferrari M, Mattavelli D. et al. Transnasal endoscopic and lateral approaches to the clivus: a quantitative anatomic study. World Neurosurg 2018; 113: e659-e671
- 15 Abouammo MD, Narayanan MS, Alsavaf MB. et al. Contralateral nasofrontal trephination: a novel corridor for a “dual port” approach to the petrous apex. Oper Neurosurg (Hagerstown) 2024; 27 (03) 347-356
- 16 Andaluz N, Van Loveren HR, Keller JT, Zuccarello M. Anatomic and clinical study of the orbitopterional approach to anterior communicating artery aneurysms. Neurosurgery 2003; 52 (05) 1140-1148 , discussion 1148–1149
- 17 Aldana PR, Naseri I, La Corte E. The naso-axial line: a new method of accurately predicting the inferior limit of the endoscopic endonasal approach to the craniovertebral junction. Neurosurgery 2012; 71 (2, Suppl Operative): ons308-ons314 , discussion ons314
- 18 Wolinsky JP, Sciubba DM, Suk I, Gokaslan ZL. Endoscopic image-guided odontoidectomy for decompression of basilar invagination via a standard anterior cervical approach. Technical note. J Neurosurg Spine 2007; 6 (02) 184-191
- 19 Visocchi M, Pappalardo G, Pileggi M, Signorelli F, Paludetti G, La Rocca G. Experimental endoscopic angular domains of transnasal and transoral routes to the craniovertebral junction: light and shade. Spine 2016; 41 (08) 669-677
- 20 Visocchi M, Di Martino A, Maugeri R, González Valcárcel I, Grasso V, Paludetti G. Videoassisted anterior surgical approaches to the craniocervical junction: rationale and clinical results. Eur Spine J 2015; 24 (12) 2713-2723
- 21 Doglietto F, Belotti F, Qiu J. et al. Endonasal and transoral approaches to the craniovertebral junction: a quantitative anatomical study. Acta Neurochir Suppl (Wien) 2019; 125: 37-44
- 22 Alsavaf MB, Abouammo MD, Gosal JS. et al. Defining the caudal limits of the endoscopic endonasal approach to the craniovertebral junction: anatomic study correlating radiographic measures. Acta Neurochir (Wien) 2025; 167 (01) 3
- 23 Fiore M, Kerr EE, Filho PM. et al. Extending the inferior limit of endoscopic endonasal surgery to the cervical spine utilizing an endoscopic endonasal posterior palatectomy. J Neurol Surg B Skull Base 2015; 76 (01) 15
- 24 Zwagerman NT, Tormenti MJ, Tempel ZJ. et al. Endoscopic endonasal resection of the odontoid process: clinical outcomes in 34 adults. J Neurosurg 2018; 128 (03) 923-931
- 25 Alijani B, Namin AK, Emamhadi M, Chabok SY, Behzadnia H, Haghani Dogahe M. Endoscopic endonasal approach to the craniovertebral junction lesions: a case series of 18 patients. J Neurol Surg B Skull Base 2022; 84 (05) 499-506
- 26 Grose E, Moldovan ID, Kilty S, Agbi C, Lamothe A, Alkherayf F. Clinical outcomes of endoscopic endonasal odontoidectomy: a single-center experience. World Neurosurg 2020; 137: e406-e415
- 27 Abouammo MD, Narayanan MS, Alsavaf MB. et al. Endoscopic total odontoidectomy with preservation of C1 anterior arch through the contralateral nasofrontal trephination technique: a cadaveric study with quantitative analysis. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 28 Mansur G, Abouammo MD, Alsavaf MB. et al. Expanding horizons in skull base surgery for the lateral recess of the sphenoid sinus: contralateral nasofrontal trephination operative video. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 29 Mansur G, Abouammo MD, Alsavaf MB. et al. Beyond traditional boundaries: a skull base morphometric cadaveric study of the novel contralateral nasofrontal trephination approach to the lateral recess of the sphenoid sinus. J Neurol Surg B Skull Base 2025; 86 (01) 348
- 30 Biswas C, Abouammo MD, Gosal J. et al. Contralateral medial transorbital corridor to the infrapetrous region as a complement to the endoscopic endonasal approach. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 31 Bhuskute GS, Gosal JS, Alsavaf MB. et al. Morphometric comparison of endoscopic endonasal transpterygoid and precaruncular contralateral medial transorbital approaches to sphenoid sinus lateral recess. Oper Neurosurg (Hagerstown) 2024; 27 (01) 96-105
- 32 Gosal JS, Bhuskute GS, Alsavaf MB. et al. Comparison of endoscopic multiport approaches to the petrous apex: contralateral transmaxillary versus contralateral medial transorbital corridor. J Neurosurg 2024; 141 (06) 1494-1504
- 33 Bhuskute GS, Gosal JS, Alsavaf MB. et al. Endoscopic precaruncular medial transorbital and endonasal multiport approaches to the contralateral skull base: a clinicoanatomical study. Neurosurg Focus 2024; 56 (04) E10
- 34 Abouammo MD, Narayanan MS, Alsavaf MB. et al. The nasopharyngo-septal butterfly flap: a novel adjunct for reconstructing large skull base defects. OTO Open 2024; 8 (04) e70016
Address for correspondence
Publication History
Received: 16 January 2025
Accepted: 21 March 2025
Accepted Manuscript online:
25 March 2025
Article published online:
12 May 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R. The expanded endonasal approach: a fully endoscopic transnasal approach and resection of the odontoid process: technical case report. Neurosurgery 2005; 57 (1, Suppl): E213 , discussion E213
- 2 Ponce-Gómez JA, Ortega-Porcayo LA, Soriano-Barón HE. et al. Evolution from microscopic transoral to endoscopic endonasal odontoidectomy. Neurosurg Focus 2014; 37 (04) E15
- 3 Visocchi M, Signorelli F, Liao C. et al. Transoral versus transnasal approach for craniovertebral junction pathologies: never say never. World Neurosurg 2018; 110: 592-603
- 4 Halderman AA, Barnett SL. Endoscopic endonasal approach to the craniovertebral junction. World J Otorhinolaryngol Head Neck Surg 2022; 8 (01) 16-24
- 5 Morales-Valero SF, Serchi E, Zoli M, Mazzatenta D, Van Gompel JJ. Endoscopic endonasal approach for craniovertebral junction pathology: a review of the literature. Neurosurg Focus 2015; 38 (04) E15
- 6 Fang CH, Friedman R, Schild SD. et al. Purely endoscopic endonasal surgery of the craniovertebral junction: a systematic review. Int Forum Allergy Rhinol 2015; 5 (08) 754-760
- 7 Gempt J, Lehmberg J, Grams AE, Berends L, Meyer B, Stoffel M. Endoscopic transnasal resection of the odontoid: case series and clinical course. Eur Spine J 2011; 20 (04) 661-666
- 8 Ottenhausen M, Alalade AF, Rumalla K. et al. Quality of life after combined endonasal endoscopic odontoidectomy and posterior suboccipital decompression and fusion. World Neurosurg 2018; 116: e571-e576
- 9 Shriver MF, Kshettry VR, Sindwani R, Woodard T, Benzel EC, Recinos PF. Transoral and transnasal odontoidectomy complications: a systematic review and meta-analysis. Clin Neurol Neurosurg 2016; 148: 121-129
- 10 Fujii T, Platt A, Zada G. Endoscopic endonasal approaches to the craniovertebral junction: a systematic review of the literature. J Neurol Surg B Skull Base 2015; 76 (06) 480-488
- 11 Joaquim AF, Osorio JA, Riew KD. Transoral and endoscopic endonasal odontoidectomies—surgical techniques, indications, and complications. Neurospine 2019; 16 (03) 462-469
- 12 Doglietto F, Qiu J, Ravichandiran M. et al. Quantitative comparison of cranial approaches in the anatomy laboratory: a neuronavigation based research method. World J Methodol 2017; 7 (04) 139-147
- 13 Doglietto F, Radovanovic I, Ravichandiran M. et al. Quantification and comparison of neurosurgical approaches in the preclinical setting: literature review. Neurosurg Rev 2016; 39 (03) 357-368
- 14 Doglietto F, Ferrari M, Mattavelli D. et al. Transnasal endoscopic and lateral approaches to the clivus: a quantitative anatomic study. World Neurosurg 2018; 113: e659-e671
- 15 Abouammo MD, Narayanan MS, Alsavaf MB. et al. Contralateral nasofrontal trephination: a novel corridor for a “dual port” approach to the petrous apex. Oper Neurosurg (Hagerstown) 2024; 27 (03) 347-356
- 16 Andaluz N, Van Loveren HR, Keller JT, Zuccarello M. Anatomic and clinical study of the orbitopterional approach to anterior communicating artery aneurysms. Neurosurgery 2003; 52 (05) 1140-1148 , discussion 1148–1149
- 17 Aldana PR, Naseri I, La Corte E. The naso-axial line: a new method of accurately predicting the inferior limit of the endoscopic endonasal approach to the craniovertebral junction. Neurosurgery 2012; 71 (2, Suppl Operative): ons308-ons314 , discussion ons314
- 18 Wolinsky JP, Sciubba DM, Suk I, Gokaslan ZL. Endoscopic image-guided odontoidectomy for decompression of basilar invagination via a standard anterior cervical approach. Technical note. J Neurosurg Spine 2007; 6 (02) 184-191
- 19 Visocchi M, Pappalardo G, Pileggi M, Signorelli F, Paludetti G, La Rocca G. Experimental endoscopic angular domains of transnasal and transoral routes to the craniovertebral junction: light and shade. Spine 2016; 41 (08) 669-677
- 20 Visocchi M, Di Martino A, Maugeri R, González Valcárcel I, Grasso V, Paludetti G. Videoassisted anterior surgical approaches to the craniocervical junction: rationale and clinical results. Eur Spine J 2015; 24 (12) 2713-2723
- 21 Doglietto F, Belotti F, Qiu J. et al. Endonasal and transoral approaches to the craniovertebral junction: a quantitative anatomical study. Acta Neurochir Suppl (Wien) 2019; 125: 37-44
- 22 Alsavaf MB, Abouammo MD, Gosal JS. et al. Defining the caudal limits of the endoscopic endonasal approach to the craniovertebral junction: anatomic study correlating radiographic measures. Acta Neurochir (Wien) 2025; 167 (01) 3
- 23 Fiore M, Kerr EE, Filho PM. et al. Extending the inferior limit of endoscopic endonasal surgery to the cervical spine utilizing an endoscopic endonasal posterior palatectomy. J Neurol Surg B Skull Base 2015; 76 (01) 15
- 24 Zwagerman NT, Tormenti MJ, Tempel ZJ. et al. Endoscopic endonasal resection of the odontoid process: clinical outcomes in 34 adults. J Neurosurg 2018; 128 (03) 923-931
- 25 Alijani B, Namin AK, Emamhadi M, Chabok SY, Behzadnia H, Haghani Dogahe M. Endoscopic endonasal approach to the craniovertebral junction lesions: a case series of 18 patients. J Neurol Surg B Skull Base 2022; 84 (05) 499-506
- 26 Grose E, Moldovan ID, Kilty S, Agbi C, Lamothe A, Alkherayf F. Clinical outcomes of endoscopic endonasal odontoidectomy: a single-center experience. World Neurosurg 2020; 137: e406-e415
- 27 Abouammo MD, Narayanan MS, Alsavaf MB. et al. Endoscopic total odontoidectomy with preservation of C1 anterior arch through the contralateral nasofrontal trephination technique: a cadaveric study with quantitative analysis. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 28 Mansur G, Abouammo MD, Alsavaf MB. et al. Expanding horizons in skull base surgery for the lateral recess of the sphenoid sinus: contralateral nasofrontal trephination operative video. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 29 Mansur G, Abouammo MD, Alsavaf MB. et al. Beyond traditional boundaries: a skull base morphometric cadaveric study of the novel contralateral nasofrontal trephination approach to the lateral recess of the sphenoid sinus. J Neurol Surg B Skull Base 2025; 86 (01) 348
- 30 Biswas C, Abouammo MD, Gosal J. et al. Contralateral medial transorbital corridor to the infrapetrous region as a complement to the endoscopic endonasal approach. J Neurol Surg B Skull Base 2025; 86 (S 01): S1-S576
- 31 Bhuskute GS, Gosal JS, Alsavaf MB. et al. Morphometric comparison of endoscopic endonasal transpterygoid and precaruncular contralateral medial transorbital approaches to sphenoid sinus lateral recess. Oper Neurosurg (Hagerstown) 2024; 27 (01) 96-105
- 32 Gosal JS, Bhuskute GS, Alsavaf MB. et al. Comparison of endoscopic multiport approaches to the petrous apex: contralateral transmaxillary versus contralateral medial transorbital corridor. J Neurosurg 2024; 141 (06) 1494-1504
- 33 Bhuskute GS, Gosal JS, Alsavaf MB. et al. Endoscopic precaruncular medial transorbital and endonasal multiport approaches to the contralateral skull base: a clinicoanatomical study. Neurosurg Focus 2024; 56 (04) E10
- 34 Abouammo MD, Narayanan MS, Alsavaf MB. et al. The nasopharyngo-septal butterfly flap: a novel adjunct for reconstructing large skull base defects. OTO Open 2024; 8 (04) e70016