

Subscribe to RSS
DOI: 10.1055/a-2500-0428
Diabetes Mellitus at an Elderly Age
Authors

The DDG clinical practice guidelines are updated regularly during the second half of the calendar year. Please ensure that you read and cite the respective current version.
Change 1:
Shortening of the text
Change 2:
Modification of recommendations for the use of OAD (glutide and gliflozin)
Thanks to good medical care in Germany, many people with diabetes mellitus now live well into old age: Of the 340,000 adults with type 1 diabetes, more than 100,000 are over 70 years of age. Approximately 8 million people have type 2 diabetes and one-fourth of this group is over 75 years of age, and approximately 1 million over the age of 80 [8].
Nationwide, there are a total of about 630,000 people with diabetes mellitus in need of care. The statements in the clinical practice guidelines are mainly directed at the majority of elderly people with type 2 diabetes and can only reflect some of the special characteristics of elderly people with diabetes. Topics such as type 1 diabetes at an elderly age, end of life, interface management or ethics are covered in the complete S2k Guideline.
The geriatric patient is defined by multimorbidity and a higher age. Age-typical functional limitations and high vulnerability create a special need for action that goes beyond blood glucose control and the management of cardiovascular risk factors or diabetes-typical complications. For differentiated therapy planning, elderly patients should be divided into functional groups ([Tab. 1]).
|
Patient group |
Patient description |
|---|---|
|
Functionally independent |
Elderly people with diabetes mellitus and good functional status. Patients with low comorbidity, at best low cognitive impairment and good compensation possibilities |
|
Functionally slightly dependent |
Elderly people with diabetes mellitus and limited functional status. Patients with multimorbidity, functional and cognitive limitations and geriatric syndromes |
|
Functionally highly dependent |
Elderly people with diabetes mellitus and extremely limited functional status or terminally ill patients. Patients with multimorbidity, geriatric symptoms, pronounced functional and cognitive limitations and the presence of diseases with limited life prognosis, e. g. terminal heart, kidney or malignant diseases |
|
End of life |
People who are on their deathbed |
A geriatric assessment should be conducted to determine resources and deficits (division into functional groups) (Practice tool 1, see Appendix).
Treatment objectives
Goals are to be agreed individually from the point of view of participatory decision-making and on the basis of the personal risk profile between doctor and patient. Resources and deficits as well as geriatric syndromes play a role. Maintaining quality of life and avoiding hypoglycaemia are the primary therapy targets. Individual aspects of quality of life should therefore be actively investigated. The HbA1c value has a lower significance in therapy decisions in older patients [2] as well as a limited informative value in renal insufficiency in such patients.
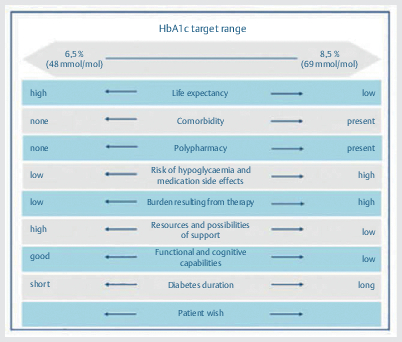
The National Care Guideline recommends an HbA1c corridor between 6.5–8.5% depending on quality of life, comorbidity, polymedication, risk of hypoglycaemia and drug side effects, burden of therapy, resources and possibilities of support, functional and cognitive abilities, duration of diabetes and patient desire (Practice tool Fig. 3).
The focus is on preventing hypoglycaemia ([Fig. 1]). The corresponding target corridors are shown in [Tab. 2]

|
Patient group |
Reasoning |
HbA1c |
Blood glucose before meals |
Blood pressure (HYVET target values apply for 80+year olds) |
|---|---|---|---|---|
(functionally independent patients) |
|
6.5–7.5% (47.5–58.5 mmol/mol) |
|
|
|
Very old, or multimorbid or slightly cognitively-impaired patients (functionally slightly dependent patients) |
|
≤ 8.0% (63.9 mmol/mol) |
|
< 150 mmHg |
|
Patients who are dependent on nursing care or cognitively severely restricted (functionally highly-dependent patients) |
Limited life expectancy |
< 8.5% (69.4 mmol/mol) |
|
Individual therapy decision that takes into account the overall context of the patient (as there is no target value evidence) |
|
End of life |
Individually with the goal of freedom of symptoms |
*Lower blood glucose limits apply only during hypoglycaemic therapy. ESC: European Society of Cardiology; ESH: European Society of Hypertension; HYVET: Hypertension in the Very Elderly Trial.
General therapy targets regarding the improvement of quality of life are contained in Practice tool 2 (see Attachment).
Individualised therapy targets should be agreed for the following parameters in elderly people with type 2 diabetes:
-
Glucose metabolism
-
Blood pressure
-
Lipid profile
Hypoglycaemias
The risk of hypoglycaemia increases with increasing duration of diabetes and is elevated in older people with diabetes [3]. The threshold for the perception of low blood glucose levels decreases with age; however, brain dysfunction occurs even at only slightly reduced levels. In addition, the symptoms of hypoglycaemia can take on a different form.
Hypoglycaemia is the second most common cause of drug-related emergency admissions of elderly people [4]. The incidence of severe hypoglycaemia is very high, at 7.8% per patient per year in nursing homes. Severe hypoglycaemia is much more common in depression, kidney and heart failure and treatment with a beta-blocker. They are most common in treatments with prandial insulin, a basal insulin or sulfonylureas or glinides; other antidiabetic treatments are associated with only a very low risk of hypoglycaemia. Elderly people with concomitant diseases, multimorbidity or impaired cognitive performance are especially at risk.
Hypoglycaemia is much more common in everyday life than previously thought, especially at night. Risk factors are long duration of illness, cognitive impairment and multimorbidity, especially renal failure. There is increasing evidence that hypoglycaemia promotes the development of cardiovascular events and dementia in old age [6]. The prevention of hypoglycaemia is a primary therapy target, especially for elderly people with diabetes. Therapy forms with the lowest possible risk of hypoglycaemia should be chosen. In people with type 2 diabetes and insulin treatment, de-escalation to therapy without the risk of hypoglycaemia should be reconsidered in the course of the disease [5].
Hypertension
-
Elderly patients benefit from effective blood pressure reduction. This also applies to patients over 80 years of age in good physical and mental condition [7].
-
There is only insufficient evidence for antihypertensive treatment in frail patients over 80 years of age, so that this therapy should be individualised (see [Tab. 1]).
-
There is no evidence for varying efficacy of antihypertensive drugs in younger or elderly patients. All major antihypertensive classes can be recommended.
Due to frequent comorbidities and polypharmacy, special attention should be paid to known adverse drug reactions in elderly patients.
Dyslipidaemia
-
In elderly patients with diabetes as well as very high risk (e. g. coronary heart disease (CHD), severe kidney damage or one or more cardiovascular (CV) risk factors and/or organ damage) a target low-density lipoprotein (LDL) cholesterol of<1.4 mmol/L (< 55 mg/dL) or an LDL cholesterol reduction ≥ 50% should be aimed for.
-
In elderly patients with diabetes without functional limitations (without other CV risk factors and without organ damage) a target LDL cholesterol of<1.8 mmol/L (< 70 mg/dL) should be aimed for [27].
-
For elderly patients with functional limitations, the use of statins should be evaluated on an individual basis.
-
Statins should be used as first-line therapy to lower LDL cholesterol.
Multi-medication
Prescription of more than five drugs increases the probability of occurrence of undesirable, clinically-relevant side effects/interactions (e. g. severe hypoglycaemia, comorbidity) and reduces patient adherence. However, it is not only multi-medication itself that should be considered. There is often a lack of indicated cardioprotective drugs if cardiovascular concomitant diseases are present in elderly patients and there is incorrect drug administration such as. e. g. overdose of psychiatric drugs or sleeping pills.
-
The treatment regimen should be based on the patient's wishes, current quality of life, as well as the individual risk and resource profile of the patient.
-
The drug therapy should be reviewed critically on a regular basis.
-
Drug dosages must be adjusted accordingly if renal insufficiency occurs, e. g. even temporarily with exsiccosis.
Assessment
Geriatric assessment refers to functional tests that are available as a diagnostic tool for recording resources and deficits and quantifying them in geriatric patients. For implementation and evaluation, etc. see www.kcgeriatrie.de.
Secondary complications
For diabetic secondary diseases, also in elderly patients, the statements by the National Healthcare Guidelines (NVL) on diabetes and retinopathy, nephropathy, diabetic foot syndrome and neuropathy generally apply. Some specifics in elderly people are highlighted below as examples:
Diabetic foot
-
Diagnostics: in contrast to monofilament examination, the examination of vibration sensation with the 128-Hertz tuning fork can be omitted in patients of advanced age.
-
Therapy: the multi-professional geriatric team is an indispensable addition in the treatment of elderly and geriatric patients with diabetic foot syndrome.
-
Prophylaxis: when selecting footwear, the risk of falling should be taken into account, e. g. in patients at risk of falling, metatarsal bars should not be used [8].
Coronary heart disease (CHD)
-
Revascularisation of coronary vessels in elderly diabetic patients remains a challenge due to the lack of randomised studies comparing percutaneous coronary intervention (PCI) with bypass surgery, especially in elderly people with diabetes.
-
Meta-analyses suggest that PCI is beneficial in elderly people with diabetes with single-vessel disease, while bypass surgery is the better choice in triple-vessel disease.
-
After exhaustion of non-drug basic therapy in clinically-relevant cardiovascular disease, primary oral hypoglycaemic agents should be used to control type 2 diabetes, which reduce the risk of the occurrence of a cardiovascular event. The German National Disease Management Guideline (Nationale VersorgungsLeitlinie, NVL) recommends a combination of metformin and sodium glucose linked transporter 2 (SGLT-2) inhibitors/or glucagon-like peptide 1 (GLP-1) receptor agonist.
Acute coronary syndrome
-
Diabetes with acute coronary syndrome is associated with a lower rate of successful coronary revascularisation and the risk of periinterventional complications in elderly people compared to younger people.
-
Insulin therapy should be started in patients with hyperglycaemia > 10 mmol/l in the acute phase of acute coronary syndrome, taking into account the comorbidities.
Stroke
-
In the context of an acute stroke, older diabetes patients with blood glucose levels > 198 mg/dl (> 11 mmol/l) should be consistently treated with insulin, as there is evidence that hyperglycaemia increases stroke volume and is associated with a poorer functional outcome.
-
In a large randomised study, intensified insulin therapy with only slightly to moderately-elevated serum glucose levels (mean 137 mg/dl (7.6 mmol/l)) had no effect on mortality and functional outcome in patients and cannot be recommended in general, especially due to the risk of hypoglycaemic episodes [9].
Therapy
Non-drug treatments are also the basis of treatment for elderly people with diabetes. In addition to the recommendations of the NVL, the following apply:
Training
Even elderly people with diabetes should participate in structured diabetes training. A special evaluated training program (SGS) is currently available for the group of functionally-impaired patients and is also available in many foreign languages [10]. If possible, relatives and friends should also participate in such a program.
Movement and tendency to fall
-
Elderly people with diabetes mellitus should be checked for a possible risk of falling.
-
In elderly people with diabetes and an increased risk of falling, medication should be reviewed with regard to drugs that increase the tendency to fall (e. g. neuroleptics, hypnotics, sedatives).
-
Elderly people with diabetes should have their visual acuity regularly checked and, if necessary and possible, they should be offered the option of correcting it.
-
Functionally mildly or severely-impaired elderly people with diabetes and their relatives should be made aware of possibilities for fall prevention and of fall hazards at home (lack of lighting, no handholds in the bathroom and near the toilet, etc.)
-
Functionally mildly or severely-impaired elderly people, especially those with frailty and diabetes, should be offered opportunities for strength and endurance training.
-
Exercise is considered the most important lifestyle measure for the prevention of dementia in advanced age.
Nutrition
-
The consequences of malnutrition are serious in advanced age. Elderly people who are overweight or obese should avoid strict dietary restrictions due to the risk of malnutrition.
-
The risk of malnutrition can be assessed using a Mini Nutritional Assessment (MNA).
-
In underweight patients, the causes should be clarified by a multi-professional team.
Oral antidiabetics and GLP-1 analogues
Advantages mentioned for the individual substances apply to monotherapy. In combination with insulin or insulinotropic substances (e. g. sulfonylureas, glinides), the increased risk of side effects (e. g. risk of hypoglycaemia) should be taken into account. Acarbose, glitazones, sulfonylureas and glinides are considered by the majority to be less suitable. The FORTA recommendations (Fit for The Aged) [11] can also be consulted for use in elderly patients.
Metformin
Metformin is also to be used as a drug therapy of first choice for elderly patients, although clinical studies on the administration of metformin in advanced age are not available (FORTA Recommendation B). In clinically-relevant renal and/or cardiovascular disease, NVL primarily recommends combination therapy of metformin plus SGLT-2 inhibitors/or GLP-1 analogues.
If metformin is used, patients should be carefully advised to discontinue/pause metformin in situations where there is a risk of acute deterioration in kidney function (such as examinations with X-ray contrast agents, surgery under general anaesthesia, febrile diseases, exsiccosis or gastrointestinal infections). Metformin can be prescribed up to a glomerular filtration rate of > 30 ml/min in a maximum dose of 1000 mg, divided into two single doses. Vitamin B12 deficiency may occur after prolonged metformin intake.
Dipeptidyl peptidase 4 (DPP-4) inhibitors
DPP-4 inhibitors can be used in elderly patients, according to FORTA first choice (Recommendation A) for elderly patients [11]. Advantages can be seen in particular with regard to therapy adherence (low frequency of administration required), risk of hypoglycaemia, weight neutrality and higher degree of renal failure (dose reduction).
GLP-1 analogues
GLP1 analogues can be used in elderly patients especially if an insulin resistance is present (SIRD) (FORTA Recommendation B). Advantages can include: low risk of hypoglycaemia, weight loss – if this is also the therapy target [12]; for liraglutide, dulaglutide and semaglutide [13] [14]: reduced cardiovascular morbidity and mortality; for dulaglutide and semaglutide [16]: administration once a week. Dulaglutide and semaglutide are available in higher dosages. Pre-filled syringes of dulaglutide are easy-to-use. Semaglutide is also available in pill form. Tirzepatide may be associated with greater weight loss, which is not always desirable in the elderly.
The NVL Type 2 Diabetes Guideline recommends the use of GLP-1 analogues in cases of clinically-relevant cardiovascular comorbidity. GLP-1 analogues should be selected that reduce the desired cardiovascular endpoint [15]. GLP-1 analogues can lead to weight reduction, which is undesirable in frailty.
SGLT-2 inhibitors
SGLT-2 inhibitors can be used in elderly patients [28]. In clinically-relevant cardiovascular disease, an SGLT-2 inhibitor should be used in combination with metformin as a first-line therapy if non-drug measures are not sufficient to achieve the individual therapy target.
Advantages can include: Lowering of blood glucose levels without personal risk of hypoglycaemia and reduced cardiovascular morbidity and mortality, avoidance of hospitalisation due to heart failure as well as a nephroprotective effect in patients with type 2 diabetes [17] [18]. During use, attention should be paid to increased risks, e. g. for urogenital infections, polyuria, exsiccosis and deterioration of renal function as well as the (rare) occurrence of (normoglycemic) ketoacidosis, especially with infection, volume and carbohydrates or lack of insulin [30] and Fournier gangrene. SGLT-2 inhibitors have an antihypertensive effect. SGLT-2 inhibitors lead to weight loss, which is undesirable in frailty.
For metformin and SGLT-2 inhibitors, the recommendation to pause the medication in times of increased stress (as with taking “sick days”) has proven to be effective.
Empagliflozin or dapagliflozin must not be used for the treatment of patients with type 1 diabetes [29].
Insulin
-
Insulin therapy should be started if lifestyle changes and/or oral antidiabetics do not achieve the individualised therapy target or oral antidiabetics are no longer effective due to contraindications or if polypharmacy can be reduced.
-
Before insulin therapy, it should be decided whether insulin should be given as monotherapy or in combination with oral antidiabetics. The choice of insulin therapy depends primarily on the patient's wishes, cognitive and fine motor skills as well as the social environment and the therapy target.
-
The money counting test [19] is suitable for assessing whether independent insulin therapy can be successful.
The following apply especially to geriatric patients: short-acting insulins (normal and analogue insulins):
Rapid-acting insulins (normal and analogue insulins):
-
For safety reasons, all rapid-acting insulins can be administered without an injection-to-meal interval or after the start of a meal in the case of loss of appetite or dementia.
Long-acting insulins (neutral protamine Hagedorn [NPH] and analogue insulins):
-
The rate of nocturnal hypoglycaemia is lower among analogue basal insulins with a normoglycemic therapy target than among NPH insulins [21]. Cloudy NPH insulins have the disadvantage that they must be mixed well before injection.
-
Provided that the patient consumes regular meals and exercises, mixed insulins can be used if fewer injections and blood glucose tests are desired.
-
Insulin degludec can be injected at variable injection times, which makes it easier to administer e. g. by nursing services.
-
De-escalation of insulin therapy should be tested in people with type 2 diabetes in the following situations:
-
If the indication (e. g. acute illness, metabolic lapse, deterioration of kidney function) is no longer present,
-
The target values of glucose metabolism are reached or not reached,
-
Hypoglycaemic events occur,
-
The individual therapy target changes (e. g. as a result of multimorbidity) [5].
-
The care of patients in domestic and long-term inpatient care
Complex insulin therapy regimens are often used at an advanced age with too strict a setting. At the same time, there is insufficient communication between general practitioners and nurses regarding insulin therapy, and emergency instructions are rarely present.
Technology
Technical aids for diabetes management for the elderly have been on the market for many years. While mechanical aids such as age-appropriate blood glucose meters or age-appropriate insulin pens are already well-established and well-accepted, electronic aids (e. g. pillboxes with reminder function) or supporting tools (PC programs or apps) have not yet found widespread use.
The evaluation of individual aids can be found in Practice tool 4 (see Appendix).
Blood glucose self-monitoring
Blood glucose self-monitoring should be carried out individually and within the scope of the possibilities (self-care competence) of the patient and the relatives or caregivers.
In the case of strongly fluctuating blood glucose levels and in a transition phase, the use of flash glucose monitoring (FGM)/continuous glucose monitoring (CGM) is also helpful in older people with diabetes and improves the quality of life.
Geriatric syndromes and special situations in advanced age
Frailty and sarcopenia
Frailty and sarcopenia are two geriatric syndromes which are of great importance for the preservation of functionality, independence, and quality of life of the elderly.
Frailty is a multidimensional syndrome characterised by decreased functional reserves, reduced resistance to stresses and increased vulnerability to negative health events such as falls, institutionalisation and mortality [22]. Frailty is diagnosed on the basis of five criteria (Practice tool) that describe a physical phenotype.
Sarcopenia is the age-associated loss of muscle mass and muscle function, often associated with weakness and the risk of falling. Both occur more frequently in elderly people with diabetes than in the population without diabetes.
-
Sarcopenia/frailty screening should be performed in elderly patients with diabetes.
-
An optimised diet and adapted training programs should be the basis of therapy for sarcopenia and frailty.
-
In patients with an increased rate of falls and fractures, measures should be taken to prevent falls.
Depression
Depression is a common mental disorder among elderly people with diabetes. A bidirectional relationship is present as well as a mutual negative influence on physical activity, compliance/adherence, or dementia [23]. With some limitations, elderly patients with diabetes can be treated in the same way as younger patients.
-
Elderly people with diabetes should be screened for depression once a year. If the result is positive, a validated, age-specific procedure should be performed.
-
Elderly people with diabetes and depression should pay particular attention to signs of possible suicidal tendencies due to the increased risk of suicide.
-
Interventions that promote physical activity and social contacts should be used in treating depression.
Dementia
In Germany there are currently about 1.7 million people with dementia. People with type 2 diabetes have a higher risk of dementia in advanced age compared to people without diabetes [24]. Dementia has a negative impact on other geriatric syndromes, especially frailty, and is associated with poorer metabolic control and an increased risk of hypoglycaemia.
-
In elderly people with diabetes, a screening of cognitive ability should be performed once a year using a validated method.
-
The cognitive requirements of diabetes treatment should be adapted to the cognitive ability of the person with diabetes.
-
Training measures should be adapted to the cognitive abilities of people with diabetes. In addition, the complexity of the content and level of language taught should be adapted accordingly.
-
Activating the body and encouraging physical activity should be encouraged within the existing physical abilities of an elderly person with diabetes and dementia.
Urinary incontinence
-
Diabetic cystopathy is often associated with diabetic neuropathy [25]. Due to polyneuropathy, examination of bladder function is always useful.
-
Elderly people with diabetes should have an incontinence assessment at least once a year.
-
Indwelling catheters should be avoided if possible; an indication for an indwelling catheter for urinary incontinence is only given if all other options fail, are rejected or cannot be applied.
Special features in care
-
The planning and evaluation of care should always be evidence-based and should incorporate current expert standards German Network for Quality Development in Nursing (DNQP) and interdisciplinary care guidelines Association of the Scientific Medical Societies in Germany (AWMF).
-
Screening/assessment tools should be shared in the exchange of information across the different areas of care (primary care, hospital, outpatient, and long-term inpatient care, etc.).
-
The care focus of geriatric patients with diabetes should include the following: avoidance of hypoglycaemia, prevention of diabetic foot syndrome, detection of pain (especially with regard to polyneuropathies), monitoring of the skin, wound assessment, wound management, and promotion of oral health, recording of the nutritional situation, preservation and promotion of continence and detection of mobility restrictions/danger of falling.
-
Nursing documentation should always be used in joint case planning across occupational groups.
-
When insulin or insulinotropic drugs (especially sulfonylureas) are administered, sufficient food intake should be ensured to avoid hypoglycaemia. When using insulinotropic drugs in nursing homes/outpatient care, it is advisable to provide instructions for the caregivers in the event of an acute complication such as severe hypoglycaemia. In case of severe hypoglycaemia (with loss of consciousness), nasal glucagon can be easily administered by first aiders.
-
Elderly people with diabetes who carry out their insulin therapy and metabolic control themselves should be regularly assessed for their cognitive and sensorimotor abilities, especially when they are adjusting or changing their therapy. Certain tests from geriatric assessment are suitable for this purpose.
The proportion of diabetes patients among the elderly of at least 25–30% is very high across all care facilities, outpatient services, homes, and clinics. At the same time, access to diabetological expertise for this patient group is low and not guaranteed for all regions. In order to ensure that diabetes patients in need of care are provided with guideline-based care no matter their location, a separate training pillar “Diabetes Care” has been added to the training program of the German Diabetes Society (DDG). The continuing education pillar consists of a basic qualification as well as continuing education to become a DDG diabetes care specialist with additional designation of the field of activity “long-term” or “clinical” (see www.deutsche-diabetes-gesellschaft.de).
Since the majority of people in need of care with diabetes are cared for at home by relatives, it is also important to provide these relatives with a special diabetes training offer. Currently, only one training program for relatives “Dia Life” of the Association of Diabetes Educators and Training Professions (Verband der Diabetes-Beratungs- und Schulungsberufe in Deutschland e. V. (VDBD)) (see www.vdbd.de) is under evaluation. Diabetes content is also included in small parts in the Allgemeine Ortskrankenkasse (AOK)-funded family care (www.aok.de/gp/pflegekurse).
Appendix: Practice tools
Practice tool 1 Procedure for geriatric assessment and its importance for the domains of diabetes treatment
|
Area |
Distinctive characteristics |
Test procedure |
Concise and practical |
|---|---|---|---|
|
Training |
Cognition testing, special curriculum/media required, training of relatives and caregivers/nursing care staff |
Visual acuity, hearing, clock-completion test, Mini Mental State Examination (MMSE) (acc. to Folstein), timed test of money counting, DemTect, Geriatric Depression Scale (GDS) |
Clock-completion test, timed test of money counting |
|
Movement |
Exercise therapy made difficult, realistic recommendations (walking) useful, effects on bones, fall/fractures, cognition |
Timed Up & Go, five-chair-rise, Short Physical Performance Battery (SPPB), Tinetti Test |
Timed Up & Go |
|
Nutrition |
Frequent malnutrition in advanced age, usual nutritional recommendations (whole grain, losing weight) not reasonable, realistic recommendations necessary for everyday life |
Condition of dentures, endoscopic evaluation of swallowing, Mini-Nutritional Assessment (MNA), NRS 2002 |
MNA screening |
|
Pharmacotherapy |
Consider polypharmacy and susceptibility to iatrogenic damage, compliance is determined by cognition and depression, insulin administration when necessary |
Check of the ability to take medication, timed test of money counting |
Practice tool 2 General therapy targets in terms of improving the quality of life
-
Avoidance of acute complications (especially hypoglycaemia)
-
Minimisation of the side effects of the therapy (e. g. severe hypoglycaemia) and of stress on the patient caused by the therapy (avoidance of polypharmacy)
-
Reduction of geriatric syndromes
-
Increasing the competence (empowerment) of those affected in dealing with the disease
-
Reduction of a disease stigma
-
Treatment satisfaction
-
Promotion of therapeutic adherence through individually-adapted therapy
-
Regular monitoring of the understanding of therapy (cognitive, sensorimotor, psychological) and the individual options
-
Prevention and treatment of symptoms by improving the metabolic control
-
Treatment and improvement of comorbidities
-
Avoidance of overtreatment by reducing polypharmacy where possible
-
Checking medication lists for missing medication if, for example, cardiovascular or renal events with subsequent impairment of quality of life can thus be prevented
-
Avoidance of overdiagnosis, where possible
Practice tool 3 HbA1c target corridor
The NVL Type 2 Diabetes Guideline provides a corridor for the HbA1c target areas, which is based on the following parameters: Life expectancy, comorbidity, polypharmacotherapy, risk of hypoglycaemia and drug interactions, burden of therapy, resources and possibilities of support, functional and cognitive abilities, duration of diabetes, patient's wishes ([Fig. 2]). It is very noteworthy that for the first time, aspects and problem areas of the elderly with diabetes are explicitly included in a national care guideline, in particular, the criteria “polymedication” and “functional and cognitive abilities”, which often affect the geriatric patient ().
Practice tool 4 Technology for the elderly
Mechanical aids:
-
Magnifying glasses and other visual aids, speaking BG measuring device (very suitable)
-
BG meters which do not require calibration, with a large display and easy operation (very suitable)
-
Insulin pens with easy release and low thumb pressure (very suitable)
-
Step-by-step instructions integrated into everyday objects (very suitable)
-
Pillboxes with weekly supply (very suitable)
Technical aids for elderly people with diabetes in a broader sense:
-
Automatic blood pressure monitors, preferably with upper arm cuff and electric pump
-
Walking aids for polyneuropathy and/or frailty (e. g. walking frame, walker)
-
Fracture prevention (e. g. safe hip protection pants, anti-slip socks)
Electronic aids:
-
PC programs for analysing collected measured values and data (partly suitable)
-
Apps to improve therapy compliance (partially suitable)
-
Apps for data management and BG control (partly suitable)
-
Technical aids to remind patients to take medication or inject insulin (partially suitable)
-
Automatic lighting with motion sensors to prevent falls (very suitable)
-
Sensor mats or Radio Frequency Identification (RFID)/Global Positioning System (GPS) systems to improve safety, for example in the case of dementia (limited suitability)
-
Flash glucose monitoring (FGM) sensors are easy to use even for elderly people with diabetes and can lead to improved blood glucose control and better quality of life.
-
Continuous glucose monitoring (CGM) systems are only suitable for some elderly people due to more complex operation
-
FGM and CGM systems, especially when integrated into electronic patient records, can make an important contribution to continuous and better metabolic control of people requiring care with diabetes and on insulin therapy in outpatient and inpatient facilities. This would make it possible to carry out therapy corrections in good time and avoid unnecessary hospital admissions.
German Diabetes Association: Clinical Practice Guidelines
This is a translation of the DDG clinical practice guideline published in Diabetologie 2024; 19 (Suppl 2): S226-235.DOI: 10.1055/a-2312-1137
Conflicts of interest
A. Bahrmann received lecture fees from the companies Bayer, Böhringer Ingelheim, Pfizer, Daiichi Sankyo, Lilly, Novo-Nordisk, Novartis and Sanofi-Aventis. AB is on the Sanofi-Aventis Advisory Board. A. Zeyfang has received lecture fees from Berlin-Chemie, Boehringer-Ingelheim, Lilly, Novo-Nordisk and Sanofi-Aventis. J. Wernecke has received lecture fees from Pfizer, Novo-Nordisk, Sanofi-Aventis, Novartis, Chiesi and Boehringer Ingelheim.
-
References
- 1 Bahrmann A, Bahrmann P, Baumann J. et al. AWMF S2k-Leitlinie Diabetes im Alter, S2k-Leitlinie Diagnostik, Therapie und Verlaufskontrolle des Diabetes mellitus im Alter. Diabetol Stoffwechs 2018; 13: 423-489
- 2 Wernecke J, Bahrmann A, Zeyfang A. Individuelle Therapieziele bei betagten Diabetespatienten. Diabetologe 2012; 8: 108-112
- 3 Hodeck K, Tittel SR, Dreyhaupt I. et al. Charakteristika von Diabetespatienten mit und ohne Pflegebedürftigkeit. Diabetol Stoffwechs 2020; 15: 392-399
- 4 Budnitz DS, Lovegrove MC, Shehab N. et al. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 2011; 365: 2002-2012
- 5 Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale Versorgungsleitlinie Typ-2-Diabetes – Teilpublikation der Langfassung. 2021; 2. Auflage. Version1
- 6 Lacy ME, Gilsanz P, Eng CH. et al. Severe Hypoglycemia and Cognitive Function in Older Adults With Type 1 Diabetes: The Study of Longevity in Diabetes (SOLID). Diabetes Care 2019; 43: 541-548
- 7 Beckett NS, Peters R, Fletcher AE. for the HYVET Study Group et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358: 1887-1898
- 8 Bahrmann A, Wernecke J. Der geriatrische Patient mit diabetischem Fußsyndrom. Diabetologe 2022; 18: 225-231
- 9 Kansagara D, Fu R, Freeman M. et al. Intensive insulin therapy in hospitalized patients: a systematic review. Ann Intern Med 2011; 154: 268-282
- 10 Zeyfang A, Feucht I, Fetzer G. et al. Eine strukturierte geriatrische Diabetiker-Schulung (SGS) ist sinnvoll. Diabetol Stoffwechs 2001; 10: 203-207
- 11 Wehling M, Burkhardt H. Hrsg. Arzneimitteltherapie für Ältere. 5. Aufl. Heidelberg: Springer; 2019
- 12 Pfeffer MA, Claggett B, Diaz R. for the ELIXA Investigators et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N Engl J Med 2015; 373: 2247-2257
- 13 Marso SP, Daniels GH, Brown-Frandsen K. for the LEADER Steering Committee on behalf of the LEADER Trial Investigators et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016; 375: 311-322
- 14 Marso SP, Bain SC, Consoli A. for the SUSTAIN-6 Investigators et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016; 375: 1834-1844
- 15 Holman RR, Bethel A, Mentz RJ. for the EXSCEL Study Group et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2017; 377: 1228-1239
- 16 Gerstein HC, Colhoun HM, Dagenais GR. et al. Dulaglutide an cardiovascular outcomes in type 2 diabetes (REWIND). Lancet 2019; 394: 121-130
- 17 Zinman B, Wanner Ch, Lachin JM. for the EMPA-REG OUTCOME Investigators et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015; 373: 2117-2128
- 18 Perkovic V, Jardine MJ, Neal B. et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med 2019; 380: 2295-2306
- 19 Zeyfang A, Berndt S, Aurnhammer G. et al. A short easy test can detect ability for autonomous insulin injection by the elderly with diabetes mellitus. J Am Med Dir Assoc 2012; 13: 81.e15-81.e8.1E18
- 20 . McMurray JJV, Solomon SD, Inzucchi SE. et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019; 381: 1995-2008
- 21 Rosenstock J, Dailey G, Massi-Benedetti M. et al. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care 2005; 28: 950-955
- 22 Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci 2007; 62: 722-727
- 23 Kulzer B, Albus C, Herpertz S. et al. Psychosoziales und Diabetes – Teil 1. S2-Leitlinie Psychosoziales und Diabetes – Langfassung. Diabetol Stoffwechs 2013; 8 . 198-242 Teil 2. Diabetol Stoffwechs 8: 292-324
- 24 Cheng G, Huang C, Deng H. et al. Diabetes as a risk factor for dementia and mild cognitive im-pairment: a meta-analysis of longitudinal studies. Intern Med J 2012; 42: 484-491
- 25 Jackson SL, Scholes D, Boyko EJ. et al. Urinary incontinence and Diabetes in Postmeopausal Women. Diabetes Care 2005; 28: 1730-1738
- 26 Deutsche Gesellschaft für Kardiologie – Herz-und Kreislaufforschung e.V. Hrsg. ESC/EAS Pocket Guidelines. Diagnostik und Therapie der Dyslipidämien, Version 2019. Grünwald: Börm Bruckmeier Verlag GmbH; 2020
- 27 Mach F, Baigent C, Catapano AL. ESC Scientific Document Group et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J 2020; 41: 111-188
- 28 Fachinformation Jardiance Böhringer Ingelheim Stand Juli 2022.
- 29 Therapie des Typ-1-Diabetes. S3-Leitlinie der Deutschen Diabetes Gesellschaft (DDG). Version 5.0. AWMF-Registernummer: 057-013. 2023
- 30 Baek HS, Jeong C, Yang Y. et al. Diabetic Ketoacidosis as an Effect of Sodium-Glucose Cotransporter 2 Inhibitor: Real World Insights. Diabetes Metab J 2024; 48: 1169-1175
Correspondence
Publication History
Article published online:
06 May 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Bahrmann A, Bahrmann P, Baumann J. et al. AWMF S2k-Leitlinie Diabetes im Alter, S2k-Leitlinie Diagnostik, Therapie und Verlaufskontrolle des Diabetes mellitus im Alter. Diabetol Stoffwechs 2018; 13: 423-489
- 2 Wernecke J, Bahrmann A, Zeyfang A. Individuelle Therapieziele bei betagten Diabetespatienten. Diabetologe 2012; 8: 108-112
- 3 Hodeck K, Tittel SR, Dreyhaupt I. et al. Charakteristika von Diabetespatienten mit und ohne Pflegebedürftigkeit. Diabetol Stoffwechs 2020; 15: 392-399
- 4 Budnitz DS, Lovegrove MC, Shehab N. et al. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 2011; 365: 2002-2012
- 5 Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale Versorgungsleitlinie Typ-2-Diabetes – Teilpublikation der Langfassung. 2021; 2. Auflage. Version1
- 6 Lacy ME, Gilsanz P, Eng CH. et al. Severe Hypoglycemia and Cognitive Function in Older Adults With Type 1 Diabetes: The Study of Longevity in Diabetes (SOLID). Diabetes Care 2019; 43: 541-548
- 7 Beckett NS, Peters R, Fletcher AE. for the HYVET Study Group et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358: 1887-1898
- 8 Bahrmann A, Wernecke J. Der geriatrische Patient mit diabetischem Fußsyndrom. Diabetologe 2022; 18: 225-231
- 9 Kansagara D, Fu R, Freeman M. et al. Intensive insulin therapy in hospitalized patients: a systematic review. Ann Intern Med 2011; 154: 268-282
- 10 Zeyfang A, Feucht I, Fetzer G. et al. Eine strukturierte geriatrische Diabetiker-Schulung (SGS) ist sinnvoll. Diabetol Stoffwechs 2001; 10: 203-207
- 11 Wehling M, Burkhardt H. Hrsg. Arzneimitteltherapie für Ältere. 5. Aufl. Heidelberg: Springer; 2019
- 12 Pfeffer MA, Claggett B, Diaz R. for the ELIXA Investigators et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N Engl J Med 2015; 373: 2247-2257
- 13 Marso SP, Daniels GH, Brown-Frandsen K. for the LEADER Steering Committee on behalf of the LEADER Trial Investigators et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016; 375: 311-322
- 14 Marso SP, Bain SC, Consoli A. for the SUSTAIN-6 Investigators et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016; 375: 1834-1844
- 15 Holman RR, Bethel A, Mentz RJ. for the EXSCEL Study Group et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2017; 377: 1228-1239
- 16 Gerstein HC, Colhoun HM, Dagenais GR. et al. Dulaglutide an cardiovascular outcomes in type 2 diabetes (REWIND). Lancet 2019; 394: 121-130
- 17 Zinman B, Wanner Ch, Lachin JM. for the EMPA-REG OUTCOME Investigators et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015; 373: 2117-2128
- 18 Perkovic V, Jardine MJ, Neal B. et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med 2019; 380: 2295-2306
- 19 Zeyfang A, Berndt S, Aurnhammer G. et al. A short easy test can detect ability for autonomous insulin injection by the elderly with diabetes mellitus. J Am Med Dir Assoc 2012; 13: 81.e15-81.e8.1E18
- 20 . McMurray JJV, Solomon SD, Inzucchi SE. et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019; 381: 1995-2008
- 21 Rosenstock J, Dailey G, Massi-Benedetti M. et al. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care 2005; 28: 950-955
- 22 Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci 2007; 62: 722-727
- 23 Kulzer B, Albus C, Herpertz S. et al. Psychosoziales und Diabetes – Teil 1. S2-Leitlinie Psychosoziales und Diabetes – Langfassung. Diabetol Stoffwechs 2013; 8 . 198-242 Teil 2. Diabetol Stoffwechs 8: 292-324
- 24 Cheng G, Huang C, Deng H. et al. Diabetes as a risk factor for dementia and mild cognitive im-pairment: a meta-analysis of longitudinal studies. Intern Med J 2012; 42: 484-491
- 25 Jackson SL, Scholes D, Boyko EJ. et al. Urinary incontinence and Diabetes in Postmeopausal Women. Diabetes Care 2005; 28: 1730-1738
- 26 Deutsche Gesellschaft für Kardiologie – Herz-und Kreislaufforschung e.V. Hrsg. ESC/EAS Pocket Guidelines. Diagnostik und Therapie der Dyslipidämien, Version 2019. Grünwald: Börm Bruckmeier Verlag GmbH; 2020
- 27 Mach F, Baigent C, Catapano AL. ESC Scientific Document Group et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J 2020; 41: 111-188
- 28 Fachinformation Jardiance Böhringer Ingelheim Stand Juli 2022.
- 29 Therapie des Typ-1-Diabetes. S3-Leitlinie der Deutschen Diabetes Gesellschaft (DDG). Version 5.0. AWMF-Registernummer: 057-013. 2023
- 30 Baek HS, Jeong C, Yang Y. et al. Diabetic Ketoacidosis as an Effect of Sodium-Glucose Cotransporter 2 Inhibitor: Real World Insights. Diabetes Metab J 2024; 48: 1169-1175