

Subscribe to RSS
DOI: 10.1055/a-2211-6841
Anti-Thrombin IgA in a Patient with Multiple Myeloma Leading to In Vitro Interference in Multiple Coagulation Tests and Confounding Diagnosis
Authors
Funding Not applicable.

Abstract
Background
We report the case of a 59-year-old multiple myeloma patient in whom an anti-human thrombin IgA antibody led to prolonged in vitro coagulation times, suggesting inhibitors to all intrinsic coagulation factors in the absence of spontaneous bleeding.
Methods
Routine and extensive special coagulation tests, in vivo bleeding time, and specific antibody testing were performed.
Results
Although the patient did not suffer from spontaneous bleeding and had a normal in vivo bleeding time, the anti-human thrombin IgA autoantibody affected all coagulation assays involving human thrombin in vitro, mimicking inhibitors to intrinsic coagulation factors. As the IgA paraprotein and the IgA antibody virtually disappeared after autologous stem cell transplantation, the coagulation tests also largely normalized.
Conclusion
Antibodies to human thrombin may interfere with all coagulation assays involving thrombin, imitating a severe coagulopathy. However, in vivo they do not necessarily lead to strongly increased bleeding tendency. Complex and ambiguous coagulation abnormalities should be evaluated and treated in an interdisciplinary setting, including a highly specialized coagulation laboratory, from the beginning.
Zusammenfassung
Wir berichten über eine 59-jährige Myelom-Patientin, die einen IgA Autoantikörper gegen humanes Thrombin entwickelt hat. Dieser führte in vitro zu verlängerten Gerinnungszeiten und täuschte Hemmkörper gegen sämtliche intrinsische Gerinnungs-Einzelfaktoren vor, wobei die Patientin keine spontane Blutungsneigung aufwies. Der Autoantikörper beeinflusste dabei alle Gerinnungstests, in welchen humanes (nicht aber bovines) Thrombin zum Einsatz kommt. Nachdem das IgA Paraprotein und somit auch der Autoantikörper nach autologer Stammzelltransplantation im Wesentlichen verschwunden war, normalisierten sich auch die Gerinnungsanalysen weitgehend. Zusammenfassend zeigt sich, dass Autoantikörper gegen humanes Thrombin zahlreiche Gerinnungstests in vitro massiv stören können ohne zwangsweise mit einer spontanen Blutungsneigung einhergehen zu müssen. Komplexe oder ungewöhnliche Konstellationen von Gerinnungsanalysen sollten von Anfang an interdisziplinär und in Zusammenarbeit mit einem hochspezialisierten Gerinnungslabor abgeklärt und behandelt werden.
Introduction
Multiple myeloma (MM) is a hematologic cancer characterized by proliferation of plasma cells in the bone marrow and suppression of normal hematopoiesis.[1] Cytogenetically, MM is a heterogeneous disorder (e.g., t(4;14), 1q gain, deletion 17p) and is commonly preceded by an asymptomatic premalignant stage (monoclonal gammopathy of undetermined significance [MGUS]), and the most common signs of the disease are taken into account in the CRAB (elevated serum calcium, renal insufficiency, anemia and/or bone lesions) criteria.[2] Unfortunately, no single test can reliably distinguish premalignant plasma cells from clonal malignant MM cells.[2] In 80% of cases, monoclonal plasma cells produce a monoclonal non-IgM immunoglobulin and in 20% of cases isolated immunoglobulin light chains,[2] both of which may appear as a paraprotein gradient in serum protein electrophoresis and can be characterized by serum immunofixation or serum immunosubtraction.[3] IgM MGUS usually evolves into Waldenström macroglobulinemia and, only rarely, into MM.[2] MM patients are at increased risk of autoimmune conditions[4] and it is plausible that the secreted monoclonal immunoglobulin may directly function as autoantibody as well.
Routine coagulation screening tests include activated partial thromboplastin time (aPTT), prothrombin time (PT), fibrinogen activity, thrombin time, and, if available, coagulation factor XIII (FXIII) activity, which is not represented in the aforementioned screening assays. The evaluation of an isolated prolonged aPTT is a common and important task of a coagulation laboratory. First, the presence of anticoagulants such as vitamin K antagonists, direct oral thrombin (dabigatran)—or factor Xa (rivaroxaban, apixaban, edoxaban, betrixaban)—inhibitors, and heparins, which are known to prolong clotting times and affect all the corresponding coagulation assays,[5] must be excluded. Second, other causes must also be considered, such as the presence of lupus anticoagulant, deficiencies of one or more contacts (high-molecular-weight kininogen [HMWK], prekallikrein), and intrinsic (FVIII, IX, XI, XII) or common pathway (FX, FV, FII) coagulation factors or a specific inhibitor to one of those.[6] Acquired neutralizing autoantibodies to single coagulation factors most commonly develop secondarily in patients with severe hemophilia A (in 20–30% of cases) and hemophilia B (in <5% of cases) as an immunological response to infused coagulation factors.[7] Spontaneous development of coagulation factor inhibitors in patients with no previous history of bleeding is very rare, whereby acquired hemophilia A, characterized by an autoantibody to FVIII, is the most common form, with an incidence of 1.5 per million per year.[8] Acquired hemophilia usually leads to acute bleeding episodes.[9] However, the clinical pictures of autoantibodies to coagulation factors other than FVIII and FIX are less well characterized and may lead to different clinical presentations. Inhibitors to coagulation factors may present without underlying disease or in the setting of other autoimmune or malignant diseases, as well as in pregnancy.[10] Treatment of acquired hemophilia includes control of acute bleeding using factor bypassing agents and immunosuppression to eliminate the autoantibody.[11] Using the example of acquired hemophilia A (autoantibody to FVIII), the workflow in detecting neutralizing autoantibodies to coagulation factors in our laboratory is briefly explained. First, plasmatic coagulation screening (aPTT, PT, fibrinogen) reveals an isolated prolonged aPTT. After excluding the presence of therapeutic anticoagulants, lupus anticoagulant is ruled out by the dilute Russell's viper venom time (DRVVT) and lupus-sensitive aPTT. Measurement of intrinsic coagulation factor activities reveals a markedly reduced FVIII activity. In the so-called Bethesda assay,[12] a multistep plasma-mixing study of patient plasma with pooled normal plasma (PNP) in several dilutions incubated at 37 °C for 2 hours, the capability of patient plasma (still containing the autoantibody to FVIII) to inhibit FVIII in PNP is assessed. Inhibitor titers are expressed in Bethesda units (BU), where 1.0 BU represents the antibody concentration capable of reducing FVIII activity from 100 to 50%.
Case Report
We report the case of a 59-year-old woman who in December 2014 underwent a hallux valgus surgery in a peripheral hospital. She suffered from hematoma at the site of spinal anesthesia. Coagulation assays revealed a markedly prolonged aPTT (aPTT ratio: 2.1). Further evaluation revealed distinctly reduced FVIII (7%) and FIX (2%) activities and strong FVIII and FIX inhibitors (47 and 50 BU, respectively). A thrombin generation assay showed a significantly reduced area under the curve, consistent with a hemophilic state. Clinical screening for underlying autoimmune and malignant diseases, including extended laboratory and imaging studies, remained inconspicuous. Initially serum protein electrophoresis was not performed and the patient was diagnosed with ‘acquired hemophilia A and B’. Surgical spinal hematoma evacuation was performed under treatment with recombinant FVIIa (NovoSeven). The patient was treated with cortisone and cyclophosphamide for several months, and rituximab was given four times. Despite aggressive immunosuppression, FVIII and FIX inhibitors increased to up to 127 and 141 BU, respectively. Clinically, the patient reported only mild cutaneous hematoma after a moderate trauma while working as a farmwoman. In April 2016, she underwent a urologic operation via the right groin. She developed hematoma of the entire right upper leg the next day. In November 2016, the patient presented with clavicular pain, and she was diagnosed with IgA kappa MM. The patient got five cycles of VTD chemotherapy (bortezomib, thalidomide, and dexamethasone) and thromboembolic prophylaxis with enoxaparin despite the diagnosis of ‘acquired hemophilia A and B’. Even under prophylactic anticoagulation with low-molecular-weight heparin, the patient did not bleed spontaneously.
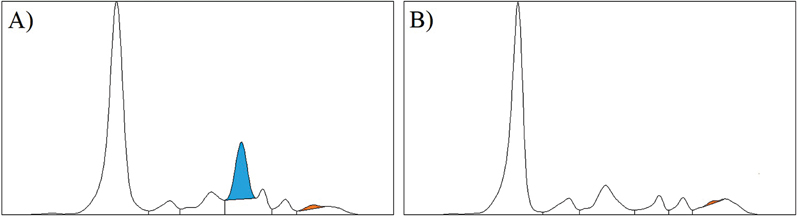
After being treated exclusively in peripheral hospitals, the patient presented for the first time at the Medical University Clinic of Innsbruck in August 2017 for evaluation for autologous stem cell transplantation (ASCT). For the assessment of ASCT risk, we performed a broad evaluation of the coagulation system. For the tests, enoxaparin was paused and the patient did not take any other anticoagulant. Coagulation tests were performed mainly on the BCS XP system (Siemens, Marburg, Germany) and reagent manufacturers and results are given in brackets or in [Table 1], respectively. In the plasma samples from August 2017, we confirmed a markedly prolonged aPTT. Additionally, three other aPTT reagents were used, thus excluding a reagent-specific effect. PT was normal and thrombin time (bovine thrombin reagent) was only minimally prolonged. On the other hand, in the argatroban-calibrated diluted thrombin time (human thrombin reagent), a considerable anti-thrombin activity was found. The anti-FXa activity assay resulted negative and all direct oral anticoagulants were excluded even with mass spectrometry. There was no evidence of lupus anticoagulant in the DRVVT and lupus-sensitive aPTT with negative confirmatory tests, and no specific antiphospholipid autoantibodies (β2-glycoprotein, cardiolipin, phosphatidylserine, phosphatidylinositol, phosphatidic acid) could be found. In the one-stage clotting assays, all aPTT-based intrinsic coagulation factors and prekallikrein were found to be below the quantification limit, while PT-based coagulation factors were only mildly reduced. Functional plasma-mixing studies suggested inhibitors against all four intrinsic coagulation factors, which in practice is very unlikely to occur. However, when chromogenic substrate assays (CSA) were used for detection of intrinsic and contact coagulation factors, all of which work by converting and measuring a chromogenic substrate proximally of thrombin within the coagulation cascade, all of them were found to be essentially normal. Of special interest was the inconspicuous chromogenic HMWK assay result, as the assay design depicts the entire intrinsic pathway until FX (HMWK → prekallikrein → FXII → FXI → FIX → FX → FXa → conversion of a chromogenic substrate). Thus, functionally highly active inhibitors against one of the intrinsic factors and thus ‘acquired hemophilia A and B’ were ruled out. Protein S activity measured functionally (depending on human thrombin) resulted <10%, while free protein S antigen determined immunologically was normal. Fibrinogen was inconspicuous both functionally and immunologically when measured with the modified Clauss method (450 mg/dL [200–400] LIAPHEN Fibrinogen, Hyphen BioMed). With antithrombin, there was a moderate discrepancy between the measurements via factor Xa (121%) and thrombin (75%). Von Willebrand antigen (187%; Siemens) and GPIb activity (140%; Siemens) as well as in vivo bleeding time (5.5 minutes [2–8 minutes]; Surgicutt, Accriva Diagnostics, San Diego, CA, United States) were normal. Testing for IgA, IgG, and IgM autoantibodies (using capture assays designed with antigen-coated micro-ELISA plates) against the following coagulation factors was performed on two different plasma samples from September 2017 at the Hyphen BioMed Experimental Laboratory: β2-glycoprotein 1, annexin V, prothrombin, protein C, protein S, protein Z, FVIII, activated FVIII, and human thrombin. Consistent with the diagnosis of IgA-kappa MM, an anti-human thrombin-IgA autoantibody was found with an estimated titer of at least 1:800, and specificity to thrombin was confirmed by the absence of reactivity to the other tested antigens. This antibody could explain almost all of the above-mentioned laboratory coagulation abnormalities. The autoantibody apparently interfered with all assays, which in any form involve human thrombin. Because of the relatively mild bleeding phenotype, it was concluded that the autoantibody did not lead to severe in vivo bleeding tendency and the patient underwent ASCT in December 2017 without complications. In February 2018, in partial remission after ASCT, the laboratory results of the patients changed distinctly when compared with a plasma sample from September 2017 ([Table 1]). IgA paraprotein markedly decreased, which was also observed in serum protein electrophoresis ([Fig. 1]). The aPTT shortened distinctly, thrombin time normalized, and no more anti-thrombin activity was detectable in the argatroban-calibrated diluted thrombin time. Furthermore, intrinsic factors measured by one-stage clotting assays and functional protein S activity became detectable. Consistently, a commercially available quantitative anti-human thrombin IgA ELISA showed a distinct decline of the autoantibody.
|
Parameter |
Reference range |
Before ASCT |
After ASCT |
Reagent; manufacturer |
|---|---|---|---|---|
|
IgA, total |
87–384 mg/dL |
979 mg/dL |
54 mg/dL |
NAS IGA; Siemens |
|
IgA, paraprotein |
– |
680 mg/dL |
20 mg/dL |
Capillarys immunotyping, Sebia, Evry, France |
|
Anti-thrombin IgA[a] |
<12 U/mL |
930 U/mL |
28 U/mL |
Thrombin IgA ELISA; IBL International, Hamburg, Germany |
|
aPTT, reagent 1[a] |
26–37 s |
71 s |
50 s |
Pathromtin SL, Siemens |
|
aPTT, reagent 2[a] |
23–32 s |
47 s |
n.a. |
Actin FS, Siemens |
|
aPTT, reagent 3[a] |
26–41 s |
93 s |
n.a. |
PTT-LA, Roche, Basel, Switzerland |
|
aPTT, reagent 4[a] |
26–41 s |
62 s |
n.a. |
CEPHEN LS, Hyphen BioMed |
|
PT, reagent 1[a] |
70–130% |
78% |
89% |
Thromborel S, Siemens |
|
PT, reagent 2[a] |
70–130% |
80% |
84% |
Thrombotest automated, Axis-Shield, Oslo, Norway |
|
Thrombin time[b] |
<21 s |
23 s |
16 s |
BC Thrombin (Bovine thrombin at <0.8 IU/mL), Siemens |
|
Argatroban-calibrated anti-thrombin activity[a] |
<0.18 µg/mL |
0.49 µg/mL |
<0.18 µg/mL |
Hemoclot thrombin inhibitors (human thrombin, 1 IU/mL, diluted thrombin time), Hyphen BioMed |
|
Fibrinogen activity[b] |
210–400 mg/dL |
410 mg/dL |
473 mg/dL |
Multifibern U (bovine thrombin at 50 IU/mL), Siemens |
|
Batroxobin time |
16–22 s |
18 s |
18 s |
Batroxobin, Siemens |
|
FII (OSA)[a] |
70–120% |
48% |
92% |
Coagulation factor-deficient plasma, Siemens |
|
FV (OSA)[a] |
70–120% |
55% |
105% |
Coagulation factor-deficient plasma, Siemens |
|
FVII (OSA)[a] |
70–120% |
49% |
82% |
Coagulation factor-deficient plasma, Siemens |
|
FVIII (OSA)[a] |
70–150% |
<1% |
56% |
Coagulation factor-deficient plasma, Siemens |
|
FVIII (chromo) |
50–200% |
197% |
148% |
Coamatic factor VIII, Chromogenix, Bedford, USA |
|
FIX (OSA)[a] |
70–120% |
<1% |
29% |
Coagulation factor-deficient plasma, Siemens |
|
FIX (chromo) |
70–130% |
56% |
97% |
Biophen factor IX, Hyphen BioMed |
|
FX (OSA)[a] |
70–120% |
44% |
64% |
Coagulation factor-deficient plasma, Siemens |
|
FXI (OSA)[a] |
70–120% |
<10% |
40% |
Coagulation factor-deficient plasma, Siemens |
|
FXI (chromo) |
65–145% |
56% |
n.a. |
Coachrom factor XI, Coachrom Diagnostica, Maria Enzersdorf, Austria |
|
FXII (OSA)[a] |
70–150% |
<10% |
32% |
Coagulation factor-deficient plasma, Siemens |
|
FXII (chromo) |
50–145% |
91% |
n.a. |
Coachrom factor XII, Coachrom Diagnostica |
|
FXIII[b] |
70–140% |
115% |
>130% |
Berichrom FXIII (bovine thrombin), Siemens |
|
Prekallikrein (aPTT-based)[a] |
70–120% |
<10% |
<10% |
Prekallikrein-deficient plasma, Cryocheck, Precision Biologic, Dartmouth, Canada |
|
Prekallikrein (chromo) |
n.a. |
150% |
n.a. |
Coachrom PKK, Coachrom Diagnostica |
|
HMWK (chromo) |
81–129% |
132% |
n.a. |
Coachrom HMW-Kininogen, Coachrom Diagnostica |
|
AT III (via FIIa)[b] |
79–112% |
78% |
111% |
Berichrom ATIII (bovine thrombin), Siemens |
|
AT III (via FXa) |
83–118% |
111% |
110% |
Innovance Antithrombin, Siemens |
|
Protein C |
70–140% |
120% |
109% |
Berichrom Protein C, Siemens |
|
Protein S activity[a] |
58–114% |
<10% |
>130% |
Protein S Ac, Siemens |
|
Free protein S antigen |
67–139% |
105% |
n.a. |
Siemens INNOVANCE Free PS Ag, Siemens |
Abbreviations: aPTT, activated partial thromboplastin time; ASCT, autologous stem cell transplantation; AT III, antithrombin III; chromo, chromogenic; F, coagulation factor; HMWK, high-molecular-weight kininogen; IgA, immunoglobulin A; n.a., not available; OSA, one-stage assay.
a Refers to assays, which involve human thrombin.
b Refers to assays, which involve bovine thrombin.
The most important parameters affected are the following:
-
aPTT. In aPTT testing, clotting is initiated by adding phospholipids, a surface activator, and calcium. Any deficiency or antagonist interfering with one of the aPTT-dependent factors (HMWK, prekallikrein, FXII, FXI, FIX, FVIII, FX, FV, thrombin, and fibrinogen) or phospholipids (e.g., due to lupus anticoagulant) can lead to a prolonged clotting time. Due to the anti-thrombin activity of the patient's antibody, aPTT was repeatedly and constantly prolonged before ASCT and improved afterward.
-
Intrinsic coagulation factor assays. Conventional one-stage clotting-based single-factor testing relies on aPTT-activated measurement using specific factor-deficient pooled plasma. As aPTT was affected, intrinsic coagulation factors were massively reduced, revealing activities below the limit of detection. In CSA, single-factor activity can be assessed independently of thrombin, as within the coagulation cascade the chromogenic substrate is converted proximally of thrombin. When testing with CSA, all intrinsic factors as well as prekallikrein and HMWK were found to be normal.
-
Prekallikrein. Prekallikrein (measured based on aPTT using prekallikrein-deficient plasma) remained below the detection limit even after ASCT. However, it should be noted that according to the package insert of the assay, patient plasma deficient in FXII may give falsely low prekallikrein results. The prekallikrein-deficient plasma used in the assay was obtained from a single prekallikrein-deficient donor, and according to the quality control certificate of the product, the donor plasma had low FXII activity (35%), too. In our patient, FXII activity was still only 32% after ASCT and obviously falsely low prekallikrein levels were measured.
-
Thrombin time. After adding thrombin to the sample, coagulation time is stopped until a fibrin clot is formed. The assay we used contained bovine thrombin; so, thrombin time was only slightly prolonged by the antibody specific to human thrombin. Batroxobin time, in which fibrin polymerization is initiated by Batroxobin venom, was within the reference range.
-
Anti-thrombin activity. We used a diluted thrombin time (human thrombin reagent) to detect direct thrombin inhibitors (e.g., argatroban, dabigatran). While using the argatroban-calibrated test, we found high anti-thrombin activity in the samples before ASCT but not afterward.
-
Protein S activity. In short, functional protein S testing relies on thrombin-induced fibrinogen polymerization. Protein S activity was below the detection limit in our patient. In contrast, immunologic free protein S antigen analysis was completely normal. Protein S activity normalized after ASCT.
-
Fibrinogen. In the modified Clauss method of fibrinogen determination, plasma is brought to coagulation by a large excess of thrombin. Our assay used bovine thrombin in large excess (50 IU/mL); thus, the fibrinogen activity was found to be normal.
At a first glance, the only unexplainable results of the anti-thrombin IgA autoantibody are the reverse antithrombin discrepancy and the fact that PT and related parameters were not significantly affected. Although the thrombin-based antithrombin assay we performed uses bovine thrombin, this does not explain why the FXa-based assay result was higher as we would rather expect the opposite. Regarding PT-related results, a possible explanation could be time dependence of the antibody: The IgA anti-thrombin antibody may compete with the normal coagulation cascade. Free thrombin is present in plasma only in trace amounts. Thus, the antibody, which is specific for human thrombin (not prothrombin), can interfere with thrombin only after the coagulation process has started. Extrinsic activation is stronger than intrinsic activation, which generally can be seen in the shorter coagulation times of PT versus aPTT. Thus, the antibody has much less time to interfere with human thrombin in PT- versus aPTT-based assays. Increasing the incubation time of aPTT (first incubation time) can correct, at least partly, a prolonged aPTT when it results from contact phase factor deficiency. APTT can also be prolonged in the presence of autoantibodies to coagulation factors through the steric hindrance on phospholipid surface (like autoantibodies to prothrombin or to FV): Immune complexes bind to these phospholipids preventing or competing with the fixation of coagulation factors. However, it is unlikely that this mechanism is involved in IgA isotype autoantibodies to human thrombin. In such cases, feedback activation of the intrinsic coagulation cascade by the first trace amounts of thrombin generated is delayed. This can result from direct inhibition of thrombin, or from a steric hindrance for activation of FXI, FVIII, and FV. The laboratory data obtained strongly suggest the involvement of the latter mechanism, which can also explain the anti-thrombin activity to human thrombin (argatroban test).
A very similar case, in which an IgA antibody with anti-thrombin activity led to coagulation test abnormalities without being associated with a severe bleeding phenotype, was reported by Baglin et al.[13] Also in our patient, the distinct in vitro coagulation abnormalities resembling inhibitors against all intrinsic coagulation factors did not lead to severe or spontaneous bleeding. Initially, in fact, the patient was erroneously diagnosed with ‘FVIII and FIX inhibitors’ and treated with highly active immunosuppressive therapy, which was not able to reduce ‘FVIII and FIX inhibitors’ and the patient did not bleed spontaneously even when receiving low-molecular-weight heparin prophylaxis. The patient also did not experience relevant bleeding symptoms in the entire period after ASCT. The results suggest that the dramatic effect observed in the anti-human thrombin antibody might only be an in vitro effect. Unfortunately, the patient died in January 2021 due to severe gastroenteritis.
Taking into account the casuistry presented, we conclude that obvious and extreme in vitro versus in vivo discrepancies should prompt the consultation of highly specialized laboratories and clinicians from the beginning to avoid delays in diagnosis and treatment and ultimately to improve the prognosis of patients.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Acknowledgments
The authors thank Margit Lanthaler (Central Institute of Medical and Chemical Laboratory Diagnostics, ZIMCL, University Hospital Innsbruck) for technical support.
Authors' Contributions
C.I., L.L., and A.G. requested, performed and/or interpreted coagulation tests. J.A. performed and interpreted autoantibody studies. C.F., C.A.Ü. and C.I. got clinical data. C.I. and J.A. wrote the original draft. All authors read, revised, and approved the submitted version of the manuscript.
Ethical Approval
If case reports with less than five patients are fully anonymized, they do not require approval by the Ethics Commission at the Medical University of Innsbruck.
Consent to Participate
At the time of writing this manuscript, unfortunately the patient was already deceased.
Availability of Data and Materials
All relevant data are contained within the manuscript.
-
References
- 1 Cowan AJ, Green DJ, Kwok M. et al. Diagnosis and management of multiple myeloma: a review. JAMA 2022; 327 (05) 464-477
- 2 Rajkumar SV, Dimopoulos MA, Palumbo A. et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 2014; 15 (12) e538-e548
- 3 Mrosewski I, Urbank M. Identification of paraproteins via serum immunofixation or serum immunosubtraction and immunoturbidimetric quantitation of serum immunoglobulins in the laboratory testing for monoclonal gammopathies. Arch Pathol Lab Med 2021; 145 (12) 1552-1557
- 4 Shimanovsky A, Alvarez Argote J, Murali S, Dasanu CA. Autoimmune manifestations in patients with multiple myeloma and monoclonal gammopathy of undetermined significance. BBA Clin 2016; 6: 12-18
- 5 Gosselin RC, Adcock DM, Bates SM. et al. International Council for Standardization in Haematology (ICSH) recommendations for laboratory measurement of direct oral anticoagulants. Thromb Haemost 2018; 118 (03) 437-450
- 6 Barbosa ACN, Montalvão SAL, Barbosa KGN. et al. Prolonged APTT of unknown etiology: a systematic evaluation of causes and laboratory resource use in an outpatient hemostasis academic unit. Res Pract Thromb Haemost 2019; 3 (04) 749-757
- 7 Ljung R, Auerswald G, Benson G. et al. Inhibitors in haemophilia A and B: management of bleeds, inhibitor eradication and strategies for difficult-to-treat patients. Eur J Haematol 2019; 102 (02) 111-122
- 8 Collins PW, Hirsch S, Baglin TP. et al; UK Haemophilia Centre Doctors' Organisation. Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors' Organisation. Blood 2007; 109 (05) 1870-1877
- 9 Knoebl P, Marco P, Baudo F. et al; EACH2 Registry Contributors. Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2). J Thromb Haemost 2012; 10 (04) 622-631
- 10 Green D, Lechner K. A survey of 215 non-hemophilic patients with inhibitors to Factor VIII. Thromb Haemost 1981; 45 (03) 200-203
- 11 Hay CR, Brown S, Collins PW, Keeling DM, Liesner R. The diagnosis and management of factor VIII and IX inhibitors: a guideline from the United Kingdom Haemophilia Centre Doctors Organisation. Br J Haematol 2006; 133 (06) 591-605
- 12 Miller CH, Platt SJ, Rice AS, Kelly F, Soucie JM. Hemophilia Inhibitor Research Study Investigators. Validation of Nijmegen-Bethesda assay modifications to allow inhibitor measurement during replacement therapy and facilitate inhibitor surveillance. J Thromb Haemost 2012; 10 (06) 1055-1061
- 13 Baglin TP, Langdown J, Frasson R, Huntington JA. Discovery and characterization of an antibody directed against exosite I of thrombin. J Thromb Haemost 2016; 14 (01) 137-142
Address for correspondence
Publication History
Received: 16 August 2023
Accepted: 13 November 2023
Article published online:
01 March 2024
© 2024. Thieme. All rights reserved.
Georg Thieme Verlag KG
Stuttgart · New York
-
References
- 1 Cowan AJ, Green DJ, Kwok M. et al. Diagnosis and management of multiple myeloma: a review. JAMA 2022; 327 (05) 464-477
- 2 Rajkumar SV, Dimopoulos MA, Palumbo A. et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 2014; 15 (12) e538-e548
- 3 Mrosewski I, Urbank M. Identification of paraproteins via serum immunofixation or serum immunosubtraction and immunoturbidimetric quantitation of serum immunoglobulins in the laboratory testing for monoclonal gammopathies. Arch Pathol Lab Med 2021; 145 (12) 1552-1557
- 4 Shimanovsky A, Alvarez Argote J, Murali S, Dasanu CA. Autoimmune manifestations in patients with multiple myeloma and monoclonal gammopathy of undetermined significance. BBA Clin 2016; 6: 12-18
- 5 Gosselin RC, Adcock DM, Bates SM. et al. International Council for Standardization in Haematology (ICSH) recommendations for laboratory measurement of direct oral anticoagulants. Thromb Haemost 2018; 118 (03) 437-450
- 6 Barbosa ACN, Montalvão SAL, Barbosa KGN. et al. Prolonged APTT of unknown etiology: a systematic evaluation of causes and laboratory resource use in an outpatient hemostasis academic unit. Res Pract Thromb Haemost 2019; 3 (04) 749-757
- 7 Ljung R, Auerswald G, Benson G. et al. Inhibitors in haemophilia A and B: management of bleeds, inhibitor eradication and strategies for difficult-to-treat patients. Eur J Haematol 2019; 102 (02) 111-122
- 8 Collins PW, Hirsch S, Baglin TP. et al; UK Haemophilia Centre Doctors' Organisation. Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors' Organisation. Blood 2007; 109 (05) 1870-1877
- 9 Knoebl P, Marco P, Baudo F. et al; EACH2 Registry Contributors. Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2). J Thromb Haemost 2012; 10 (04) 622-631
- 10 Green D, Lechner K. A survey of 215 non-hemophilic patients with inhibitors to Factor VIII. Thromb Haemost 1981; 45 (03) 200-203
- 11 Hay CR, Brown S, Collins PW, Keeling DM, Liesner R. The diagnosis and management of factor VIII and IX inhibitors: a guideline from the United Kingdom Haemophilia Centre Doctors Organisation. Br J Haematol 2006; 133 (06) 591-605
- 12 Miller CH, Platt SJ, Rice AS, Kelly F, Soucie JM. Hemophilia Inhibitor Research Study Investigators. Validation of Nijmegen-Bethesda assay modifications to allow inhibitor measurement during replacement therapy and facilitate inhibitor surveillance. J Thromb Haemost 2012; 10 (06) 1055-1061
- 13 Baglin TP, Langdown J, Frasson R, Huntington JA. Discovery and characterization of an antibody directed against exosite I of thrombin. J Thromb Haemost 2016; 14 (01) 137-142