

Subscribe to RSS
DOI: 10.1055/a-2057-0205
Sarcopenia, More Than Just Muscle Atrophy: Imaging Methods for the Assessment of Muscle Quantity and Quality
Sarkopenie, mehr als nur Muskelschwund: Bildgebende Verfahren zur Beurteilung von Muskelquantität und -qualitätAuthors

Abstract
Background Sarcopenia, a progressive reduction of muscle mass and function, is associated with adverse outcomes in the elderly. Sarcopenia and muscle atrophy are not equal processes. Low muscle strength in association with muscle quantity/quality reduction is currently the optimal method for assessing sarcopenia. There is a practical need for indirect measurement of muscle strength using state-of-the-art imaging techniques.
Methods The following provides a narrative, broad review of all current imaging techniques for evaluating muscles and identifying sarcopenia, including DEXA, CT, MRI, and high-resolution ultrasound, their main strengths, weaknesses, and possible solutions to problems regarding each technique.
Results and Conclusion Well-recognized imaging methods for the assessment of muscle mass are explained, including evaluation with DEXA, CT, and MRI muscle quantity assessment, ultrasound evaluation of muscle thickness and CSA, and their correlations with established muscle mass calculation methods. A special focus is on imaging methods for muscle quality evaluation. Several innovative and promising techniques that are still in the research phase but show potential in the assessment of different properties of muscle quality, including MRI DIXON sequences, MRI spectroscopy, Diffusion Tensor Imaging, ultrasound echo intensity, ultrasound elastography, and speed-of-sound ultrasound imaging are briefly mentioned.
Key Points:
-
Sarcopenia definition includes low muscle strength and low muscle quantity/quality.
-
DEXA is a low-radiation method for whole-body composition measurement in a single image.
-
CT has established cut-off values for muscle quality/quantity evaluation and sarcopenia diagnosis.
-
MRI is the most sophisticated muscle quality assessment method capable of evaluating myosteatosis, myofibrosis, and microstructure.
-
Ultrasound can evaluate muscle quality, including tissue architecture, and elasticity with excellent spatial resolution.
Citation Format
-
Vasilevska Nikodinovska V, Ivanoski S, . Sarcopenia, More Than Just Muscle Atrophy: Imaging Methods for the Assessment of Muscle Quantity and Quality. Fortschr Röntgenstr 2023; 195: 777 – 789
Zusammenfassung
Hintergrund Sarkopenie, eine fortschreitende Abnahme der Muskelmasse und -funktion, ist bei älteren Menschen mit ungünstigem Verlauf verbunden. Sarkopenie und Muskelschwund sind keine gleichwertigen Prozesse. Eine geringe Muskelkraft in Verbindung mit einer Verringerung der Muskelquantität/-qualität ist derzeit das optimale Verfahren, um die Sarkopenie zu beurteilen. Daher besteht ein praktischer Bedarf an einer indirekten Messung der Muskelkraft mit Hilfe modernster bildgebender Verfahren.
Methoden Im Folgenden wird ein umfassender Überblick gegeben über alle aktuellen bildgebenden Verfahren zur Beurteilung von Muskeln und zur Identifizierung der Sarkopenie, darunter DEXA, CT, MRT und hochauflösender Ultraschall, über ihre wichtigsten Stärken und Schwächen sowie mögliche Lösungen für die Probleme der einzelnen Techniken.
Ergebnisse und Schlussfolgerungen Anerkannte bildgebende Verfahren zur Bewertung der Muskelmasse werden erläutert, darunter die Bewertung mit DEXA, CT und MRT zur Bestimmung der Muskelmasse, der Ultraschallbewertung der Muskeldicke und der Querschnittsfläche (CSA) sowie ihrer Korrelationen mit etablierten Verfahren zur Berechnung der Muskelmasse. Ein besonderer Fokus liegt auf den bildgebenden Verfahren zur Bewertung der Muskelqualität. Mehrere innovative und vielversprechende Techniken, die sich noch in der Forschungsphase befinden, aber Potenzial für die Bewertung verschiedener Eigenschaften der Muskelqualität zeigen, wie z. B. MRT-DIXON-Sequenzen, MRT-Spektroskopie, Diffusions-Tensor-Bildgebung, Ultraschall-Echointensität, Ultraschall-Elastografie und der Speed-of-Sound Bildgebung, werden kurz erwähnt.
Kernaussagen
-
Die Definition der Sarkopenie umfasst eine geringe Muskelkraft und eine geringe Muskelquantität/-qualität.
-
DEXA ist ein strahlungsarmes Verfahren zur Bestimmung der Ganzkörperzusammensetzung in einem einzigen Bild.
-
Für die CT wurden Cutoff-Werte für die Bewertung der Muskelqualität/-quantität und die Diagnose der Sarkopenie festgelegt.
-
Die MRT ist die fortschrittlichste Methode zur Beurteilung der Muskelqualität, mit der Myosteatose, Myofibrose und Mikrostruktur bewertet werden können.
-
Ultraschall kann die Muskelqualität, einschließlich der Gewebearchitektur, und die Elastizität mit hervorragender räumlicher Auflösung beurteilen.
Key words
sarcopenia - muscle quantity and quality - DEXA - computed tomography - magnetic resonance - ultrasoundIntroduction
Sarcopenia is a progressive reduction of muscle mass and function that appears in the elderly, but also secondary to various systemic diseases. It is associated with a poor prognosis, higher complication rate, and mortality [1]. Its prevalence fluctuates in different populations ranging between 5 % and 13 % in the those 60 to 70 years old and up to 50 % in the population older than 80, partially depending on the definition used. Nevertheless, a conservative assessment suggests that over 200 million people will be affected by the disease by 2050 [2].
The original definition of sarcopenia by Rosenberg included a reduction of muscle mass, associated with the process of ageing [3]. Muscle mass declines constantly during adulthood [4] and is connected to the reduction of muscle strength [5]. A systematic review by Rozenberg et al. [5] evaluated the extremity muscles in patients with chronic lung diseases. Results showed that muscle size measured with magnetic resonance imaging (MRI), computed tomography (CT), and ultrasound (US) correlates to muscle strength and physical performance tests. However, the reduction of muscle strength and functional impairment is not linearly correlated to a simple loss of muscle mass [4] [6]. Although muscle mass was considered a key determinant of functional ability in the elderly [7], more recent studies stress the importance of muscle strength in the characterization of functional loss [8]. Muscle strength and muscle power decline at a higher rate than muscle mass in the ageing process [4]. Evaluating changes in muscle mass and strength in elderly individuals as a function of time, Goodpaster et al. [9] showed that the muscle strength reduction was 3-fold greater compared to muscle mass decline. Preserving muscle mass in the elderly does not inhibit muscle strength reduction [6] [9]. Muscle strength is currently the most important prognostic factor for sarcopenia-related adverse outcome [10] [11] [12]. A recent definition of sarcopenia by the European Working Group for Sarcopenia in Older People (EWGSOP) highlights the importance of muscle strength over muscle mass as the essential appearance of sarcopenia. EWGSOP defines sarcopenia as low muscle strength combined with a decline in muscle quantity or quality. The physical performance level can further determine the severity of sarcopenia [10].
Muscle strength and physical performance can be measured directly with different assessment tests [13] ([Fig. 1a, b]). However, there is a practical need for an indirect measurement of muscle function [14]. Muscle quality is usually defined as the force-generating capacity of a muscle tissue unit [15]. It’s a concept developed to help overcome the discrepancies between the extent of muscle mass and muscle strength/power decline in ageing [15] [16] [17]. It is dependent on different factors, including the muscle architecture and muscle size, amount of fat and fibrous tissue within the muscle, microvascularity, motor unit, oxidative stress, muscle metabolism, and muscle contractility and fatigability [14] [18]. A reduction of muscle quality precedes and leads to reduced quality of life and functional decline in the elderly [14].

Muscle quality is considered the most important factor for identifying sarcopenia [10]. However, because of technical limitations and the lack of a standardized definition, a consensus about the optimal method/s of muscle quality assessment with the current imaging modalities has not yet been reached.
This review aims to describe the methods and imaging techniques for the assessment of muscle changes in the process of ageing, as well as the recent technical advantages that can improve the evaluation of the muscle quantity and quality and the diagnosis of sarcopenia in the near future.
A PubMed search for the term “sarcopenia”, combined with one of the words “DEXA”, “DXA”, “CT”, “MRI”, “ultrasound”, “US”, “muscle quality”, “muscle mass”, or “muscle quantity” was performed to identify possible articles. In addition, the references in the identified papers were reviewed and a random search for papers was also performed. Only studies involving humans were considered, with emphasis on research articles, systematic reviews, meta-analyses, and clinical trials.
Dual-energy X-ray absorptiometry
Dual-energy X-ray absorptiometry (DEXA) is a method of evaluating the body structure by calculating the absorption of the X-rays passing through the body at two different energy levels [19] [20]. Three different tissue composition parts can be assessed, the bone mineral content, which is measured directly, and the fat mass and fat-free mass, which are calculated indirectly. The ability to measure the composition of the whole body or extremities in a single image is a major advantage of the method compared to the other imaging modalities [20]. The radiation dose is insignificant for the adult population, ranging between 1 and 4 µSv [21], compared to a much higher average radiation dose of 8 mSv for an abdominal CT exam [22]. The EWGSOP facilitates the use of DEXA as a primary method for muscle mass assessment in clinical practice [10].
The international society for clinical densitometry recommends reporting several values in each DEXA exam besides the body mass index (BMI), bone mineral content and density, including the total mass, the total fat and total lean mass, as well as the percentage of fat mass [23]. Other parameters can be optionally measured and reported, like the lean mass index (fat-free mass index), appendicular lean mass index (ALMI), visceral adipose tissue, and fat mass index (FMI) [23].
Appendicular lean mass (ALM) is a summation of the lean mass of the upper and lower extremities. The appendicular lean mass index (ALMI) – the ALM divided by the patient height2 – is the most frequently used DEXA method for the assessment of muscle mass and diagnosis of sarcopenia [21]. Baumgartner et al. [24] were the first to establish specific cut-off values for sarcopenic ALMI using DEXA. The cut-off values were calculated as 2 SD below the average for the young healthy population and were set to 7.25 kg/m2 and 5.45 kg/m2 in men and women, respectively [24]. Several other authors used the same method to calculate cut-off values for sarcopenia, which vary somewhat in different populations [25]. DEXA-derived values for ALMI show a correlation to CT-derived muscle mass. Lindqvist et al. [26] compared the DEXA-obtained ALMI with the skeletal muscle index at the L3 vertebral level obtained by CT in patients with chronic hepatic disease and showed a strong correlation between the two methods.
There are a few disadvantages of DEXA in the evaluation of sarcopenia. Probably, the most important weakness is the inability to adequately measure the visceral and intramuscular fat [19]. The equipment is not universally available at hospitals [27]. The muscle mass values can vary due to the hydration status and can be overestimated in individuals with an excessive increase in extracellular fluid [26] [27], or in individuals with severe obesity [28]. Lidqvist et al. [26], showed that the fat-free mass index can overrate the muscle mass in patients with ascites. The problem with the DEXA muscle mass estimation in obese individuals might be overcome by dividing the ALM by the BMI instead of height2 [20] [29].
Computed Tomography
EWGSOP considers CT a gold standard method for the evaluation of muscle mass. Numerous abdominal CT exams are performed every day for the diagnosis, staging, and follow-up of neoplastic and many other diseases [30]. Each abdominal CT exam contains potentially valuable information about muscle mass, muscle and visceral fat infiltration, bone mineral density, and arterial calcifications that might be used as screening tools for predicting a future adverse outcome [31]. Opportunistic imaging uses the usual, routine imaging modalities for obtaining new imaging biomarkers and achieving additional useful information [32]. Opportunistic CT imaging has been shown to be valuable in the evaluation of myosteatosis and the diagnosis of sarcopenia. The most commonly used opportunistic CT diagnostic technique is an assessment of the muscle quantity (usually presented as muscle cross-sectional area (CSA)) and muscle radiodensity or attenuation [32] illustrating the muscle quality.
Evaluating 50 patients with a cancer diagnosis, Mourtzakis et al. [33] were the first authors to compare the CSA of all muscles included on a single CT slice at L3 vertebral level with fat-free mass assessed with DEXA. The muscle CSA was strongly correlated to the whole-body fat and fat-free mass estimated by DEXA (r = 0.88 and r = 0.83, respectively). Muscle CSA, also known as skeletal muscle area (SMA), acquired at the L3 vertebral level is the most commonly used CT method for quantifying skeletal muscle mass [34] [35], followed by mid-thigh muscle CSA and psoas CSA at the L3 or L4 vertebral level [35]. In addition, paraspinal muscle CSA at the Th12 level [36], total muscle CSA at the Th12 [37] or L1 [38] level, total CSA at the C3 vertebral level [39] [40], compared directly or adjusted with prediction formulas show significant correlations to L3 SMA.
Calculating the muscle CSA from CT images usually consists of choosing the region of interest (area containing all muscles included within the slice), and segmentation by applying threshold values, usually between -29 and 150 HU, to avoid measurement of the intermuscular fat ([Fig. 2]). The results for CSA, expressed in square centimeters, adjusted for the patient’s height by dividing it by height2, are known as the skeletal muscle index (SMI) [30].

Evaluating the effects of sarcopenic obesity in patients with gastrointestinal and lung malignancy, Prado et al. [41] showed that muscle attenuation in patients with sarcopenic obesity was significantly lower compared to attenuation in obese patients without sarcopenia (p < 0.0001), due to the increased amount of adipose tissue within muscles. Myosteatosis, a term comprising intermuscular, intramuscular, and intramyocellular adipose tissue, negatively correlates to muscle strength and function [42]. Myosteatosis precedes the functional decline of the muscle [43]. Intramuscular adipose tissue decreases the muscle quality. It can influence muscle contractility and strength directly by modifying the orientation of muscle fibers, or indirectly by the metabolic effects of the adipose tissue [43]. By evaluating over 300 patients in a geriatric center, Perkisas et al. [44] showed that CT-measured intramuscular fat tissue correlates to mortality rate as well as to muscle function and strength. The authors concluded that muscle mass in hospitalized geriatric patients might be overestimated due to fat infiltration, which should be taken into consideration in the assessment of sarcopenia.
The assessment of muscle quality by measuring myosteatosis is performed similarly to determination of the SMA on abdominal axial slices, using the same procedure of mapping and segmentation of the required anatomic region and setting the threshold values [34]. The intermuscular fat-tissue area at the L3 or mid-thigh level, using threshold values between -190 and -30 HU, is commonly used to evaluate myosteatosis [35] ([Fig. 2]). CT density values of the muscles at the mid-thigh level or psoas muscle are also useful for myosteatosis assessment [35]. Muscle attenuation on contrast-enhanced CT scans is significantly altered and dependent on several factors [45]. Therefore, non-contrast-enhanced images should always be used for the evaluation of muscle quality.
Muscle quantity or quality can be estimated manually or automatically on CT [31] by using one of the many available segmentation software products. Traditional image segmentation methods consist of manual, precise outlining of the borders of muscles or muscle groups of interest for further evaluation. It is a time-consuming method requiring vast anatomical knowledge and is costly and impractical for routine clinical evaluation, thus limiting its use mainly to scientific research. Automatic muscle area segmentation methods using artificial intelligence are evolving techniques that enable rapid, precise, and cheap image segmentation that is applicable for everyday clinical use [46]. A recent article compared manual to automated segmentation of muscular tissue as well as subcutaneous, visceral, and intermuscular adipose tissue on CT images [47]. The results confirmed the accuracy of the automatic analysis of body composition, showing excellent agreement between the two methods, with advantages of the automated analysis including reduced time and cost for the procedure.
CT-derived values for muscle mass are associated with mortality and complication rate [48]. A meta-analysis conducted by Su et al. [49] including 70 studies, evaluated the influence of sarcopenia diagnosed by CT on survival and complication rate in gastrointestinal malignancies. The muscle CSA at the L3 level, the psoas muscle cross-section, or the visceral fat area defined the cut-off values in the majority of the studies. The patients with sarcopenia had a significantly higher mortality rate (HR = 1.602) and higher complication rates (RR = 1.188) compared to non-sarcopenic patients. Another meta-analysis performed by Xia et al. [50] focused on the effect of sarcopenia in trauma patients. CT-derived SMA or muscle density was used for sarcopenia diagnosis. The mortality rate was significantly higher in patients with sarcopenia (RR = 3.11 for one-year mortality), but controversially not the length of stay or the complication rate. A meta-analysis including 14 articles evaluating the relationship between colorectal cancer and sarcopenia defined by muscle fat infiltration showed that myosteatosis is a predictor of the overall survival rate [51]. A recent article by Martin et al. showed that myosteatosis is an independent risk factor for mortality in patients with head and neck, lung, or gastrointestinal cancer [52].
The major disadvantage of CT in the assessment of sarcopenia is the radiation dose, which is the highest compared to all other imaging modalities, making the method practical only for patients undergoing CT for different diagnostic purposes [21]. CT is an expensive method, demanding highly trained operators [53]. In addition, some authors express concern that tumor cachexia leading to muscle loss (which is measured in many studies using CT) and sarcopenia are distinct conditions, modulated by different pathophysiological processes, possibly requiring diverse therapeutic strategies, so they should not be equated [54].
Magnetic resonance
MRI is a reliable method for the evaluation of muscle mass. Several MRI methods of assessing muscle quantity exist, and the most commonly used pulse sequences are T1, T2, and PD [55]. Although muscle volume determined by whole-body MRI is considered a gold standard technique for muscle quantity assessment [56], single-slice procedures in an axial plane, which are more practical and less time-consuming, are more frequently used [25]. Muscle CSA values, expressed as cm2 or divided by the patient height2, show a significant correlation to total skeletal muscle mass [25]. Common measurement sites include but are not limited to mid-thigh muscle CSA and total muscle CSA at L3 or another lumbar vertebral level [56]. Muscles or muscle groups can be demarcated manually or automatically, with the addition of segmentation software to separate the muscle from the adipose tissue [57] ([Fig. 3]). Similarly to automated CT segmentation methods, evolving automatic MRI segmentation software enables rapid and accurate image segmentation requiring less time and resources.

MRI values for muscle quantity, using several different pulse sequences, show a significant correlation and interchangeable results with CT. Sinelnikov et al. [58], for example, compared to the values for total SMA at the L1 vertebral midlevel acquired by CT and MRI sequences (T1-weighted in-phase and out-of-phase and T2-weighted). The authors showed a significant correlation between the two methods, and the T2-weighted images had the strongest correlation with CT (r = 0.98). Wang et al. [59] compared the CT and MRI values for muscle mass acquired at the L3 vertebral midlevel in 32 patients with renal diseases. MRI CSA using IDEAL-IQ sequence fat images had a significant, strong correlation with CT-derived CSA (r = 0.995). Faron et al. [60] showed results for CT-measured paraspinal muscle mass and density comparable to MRI results for the paraspinal mass and myosteatosis obtained by proton density fat fraction (PDFF).
Sarcopenia defined by MRI-obtained trunk SMA, fat-free area, or fat area in patients with additional coexisting diseases is a predictor of adverse outcome [55]. A recent study by Beer et al. [61] evaluating the outcome of sarcopenia in advanced chronic liver disease showed that patients with sarcopenia, defined by a psoas muscle transverse diameter at the L3 level, had a higher mortality risk compared to non-sarcopenic patients.
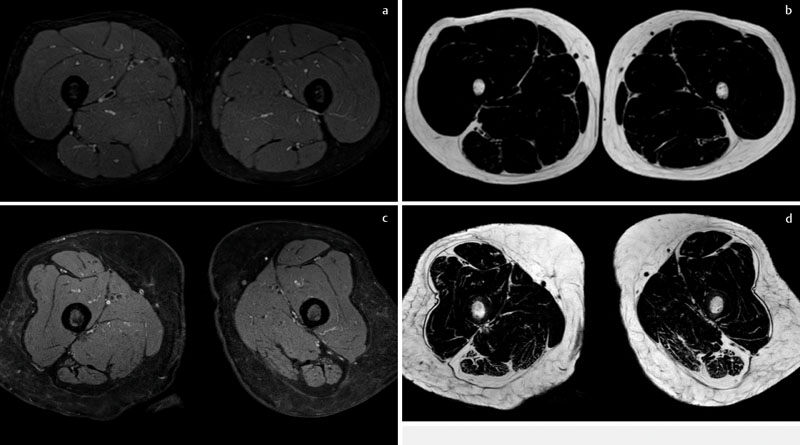
MRI is the most sophisticated existing method for the evaluation of muscle quality. Myosteatosis can be accurately measured with several MRI techniques including Dixon sequences ([Fig. 4]) or proton MR spectroscopy [62]. The majority of the studies exploring the usefulness of MRI in myosteatosis use the PDFF, obtained with Dixon T1 or T2-weighted images [55]. Dixon sequences, which are based on the chemical shift phenomenon, are capable of accurately differentiating water from fat protons and quantifying muscle fat tissue [63]. Maps of the fat fraction of large areas or volumes can be produced with the grey value of each pixel representing its fat content percentage [62] [64]. Moreover, Dixon MRI sequences using PDFF can separate intermuscular fat from intramuscular fat that might have a clinical significance [64]. A recent study by Schlaegger et al. [65], for example, examined the correlation between the PDFF of erector spine muscle and psoas muscle with their isometric muscle strength in 26 young healthy individuals. The results showed significant correlation between the erector spine muscle relative strength and PDFF (r = –0.51 in extension and r = –0.54 in flexion). Proton MR spectroscopy, on the other hand, is a noninvasive method capable of distinguishing the intramyocellular from extramyocellular lipid content [66] ([Fig. 5]). A recent study by Grimm et al. [67] showed that Dixon MRI and MR spectroscopy can quantify the fat content percentage with similar accuracy. However, several authors favor the use of Dixon MRI, due to the ease of performing and establishing maps of the fat fraction. MR spectroscopy, which is mostly a single voxel technique, can evaluate only a small fraction of muscle [63], which can be challenging for analysis because muscle is a rather heterogeneous tissue. Assessment of multiple voxels in a single acquisition, with recently available protocols, can resolve this issue [62].

The phosphorus metabolites within the cells are important for the integrity of the intracellular organelle and the accumulation of energy needed for high-energy-dependent organs [68]. The phosphocreatine within the muscles is essential as a high-energy source, necessary for short but energy-dependent muscle contractions [68]. Phospholipids are also important structural and functional parts of the mitochondrial membrane. Mitochondrial phospholipid impairment is linked to the evolution of cardiometabolic diseases [69]. Phosphocreatine and phosphodiester levels are connected to muscle mass and function properties [70]. 31-phosphorus MR spectroscopy is potentially a powerful tool for sarcopenia diagnosis since it is capable of assessing the levels of different phospholipids within the muscle cells. A study by Hinkley et al. [70] evaluated the difference in phospholipids between elderly patients with sarcopenia and nonsarcopenic individuals using 31-phosphorus MR spectroscopy. The results showed that individuals with sarcopenia had significantly lower levels of phosphocreatine and higher levels of phosphodiester.
Myofibrosis, a process involving the replacement of normal muscle tissue with excessive fibrous connective tissue and decreased regenerative potential of the muscles, accompanies the process of ageing [71]. Myofibrosis is an important factor in the reduction of muscle mass, muscle elasticity and strength, and progression of muscle atrophy [71] [72]. Myofibrosis and myosteatosis are interconnected phenomena and contribute to muscle quality reduction [71]. MRI strain rate tensor imaging can indirectly evaluate the excessive extracellular matrix deposition seen in various muscle impairment diseases, including sarcopenia [73]. Sinha et al. [73] evaluated the two-dimensional strain rate tensor during passive joint movement and isometric muscle contraction of the medial gastrocnemius muscle. The authors concluded that strain rate mapping might detect the age-related alterations of active and passive movement, probably caused by muscle contractility and elasticity differences. T2 mapping is a promising method in the evaluation of myofibrosis. Evaluating age differences of quadriceps muscles using a multi-slice multi-echo sequence, Azzabou et al. [74] showed that water T2 values and water T2 heterogeneity were significantly lower in the younger group compared to the elderly, presumably due to differences in muscle fiber types and myofibrosis in the elderly population. Diffusion tensor imaging (DTI) using parameters, such as mean diffusivity and fraction anisotropy, is an advanced method for the evaluation of muscle microstructure, although it is related to several weaknesses that need to be overcome [63]. DTI combined with fiber tractography algorithms can provide information about muscle fiber length and orientation and allow three-dimensional reconstruction of the muscle [75]. In addition, DTI parameters can detect age-related muscle alterations [76]. A recent study by Farrow et al. [77] compared the mean diffusivity (MD) between 3 different age groups of healthy participants and the correlation of the MD with the frailty index, muscle strength, muscle power, and physical function tests. The results showed significant differences in MD among the age groups and a correlation between the MD and the test results.
Although MRI is the most advanced method of muscle quality and quantity assessment, several issues restrict its use in clinical practice, including availability, the high cost of the exam, which is also time-consuming, and the requirement of highly specialized operators [53]. Image acquisition and assessment protocols for the diagnosis of sarcopenia and the cut-off values are still not established [78].
Ultrasound
Ultrasound (US) is an easily accessible, cheap, and portable method for the analysis of muscle tissue. Technical advances in US hardware, high-frequency linear transducers that offer visualization of muscle tissue with a resolution that is unavailable for any other imaging modality, and the possibility of assessing muscle elasticity make US a feasible method for tracking the changes appearing in the process of ageing.
US measurements of muscle size, thickness, and cross-sectional area show a positive correlation to the proven tests for muscle mass evaluation, including DEXA [79], bioelectrical impedance [80], CT [81], and MRI [82], but also muscle function tests [83] [84]. Sarcopenia does not affect all muscles homogeneously [85], a process known as regional sarcopenia. The muscles of the lower extremities are affected earlier by age-related loss compared to the muscles of the upper extremities [85], and the reduction of the anterior thigh muscles occurs at a higher rate compared to the other leg muscles [86]. Consequently, the majority of the studies evaluating muscle size by US pay particular attention to the quadriceps muscle and its parts [83] ([Fig. 6a, b]).

However, the loss of muscle mass is not always connected to sarcopenia. The muscle mass decline in sarcopenia and disuse atrophy are diverse processes, resulting in different changes in muscle architecture. They both include shortening of the muscle fibers, which is a reversible process. On the other hand, the reduction of the number of muscle fibers, fiber diversity, and fiber type grouping affecting muscle quality and function appears only in sarcopenia [54] [87].
The arrangement of the muscle fibers or the muscle architecture is the best predictor of functional capacity [88]. Most of the muscles in the extremities have oblique fascicles, oriented at a certain angle to the tendon direction [89] [90]. Such muscles, also known as pennate muscles, have greater force-generating potential compared to parallel muscles [89], due to the packing of more contractile tissue within the same volume unit. The ability of US to evaluate architectural changes in muscle, such as the fascicle length and pennation angle variation, is the main advantage versus other imaging modalities ([Fig. 7]). Narici et al. [91] compared the pennation angle and fiber length of the gastrocnemius medialis between physically active young people and elderly individuals. They were the first authors to show that the changes in muscle architecture seen in the elderly were primarily a consequence of the process of ageing and not disuse atrophy. The authors attributed the pennation angle decrease in the elderly group to a reduction in both fiber length and fiber number. However, there are still differing opinions about the usefulness of US for muscle architecture, probably due to the low reproducibility of the method [92]. The calf muscles that are commonly evaluated, display significant changes of the pennation angle and fascicle length during contraction or different foot positions, requiring standard procedures and trained physicians to obtain accurate results [92].

Echo intensity (EI) is defined as the average brightness of a selected US image area, which can be calculated using computer-aided analysis and expressed in grayscale from 0 to 255 [93]. Non-contractile intramuscular elements that accumulate in the process of ageing, such as fibrous and adipose tissue, increase the muscle EI [94]. EI is emphasized as a method of choice for muscle quality analysis [95]. It is a predictor of the functional status of the muscle and correlates to other methods of myosteatosis evaluation ([Fig. 8a, b]). Akima et al. [96] showed that the EI and the extramyocellular fat quantity acquired with MR spectroscopy of the rectus femoris and vastus lateralis muscles are linked. Haris-Love et al. [97] showed a significant correlation between CT-established thigh intra- and intermuscular fat and rectus femoris EI. EI in the same study also revealed a negative correlation with upper and lower extremity strength tests. Isaka et al. [98] proved that muscle thickness and EI of the tibialis anterior are associated with muscle mass and handgrip strength tests and that the combination of both measurements is a useful diagnostic tool for the diagnosis of sarcopenia.

Muscle changes can be evaluated with US elastography techniques, which can detect stress-induced tissue alterations [83] ([Fig. 9]). In particular, shear-wave elastography shows encouraging initial results for the assessment of age-related muscle differences, but also muscle function, proving its usefulness in assessing muscle quality [99]. Evaluating rectus femoris and gastrocnemius medialis muscles with shear-wave elastography, Saito et al. [100] showed a significant difference in elasticity between healthy young and senior female individuals. Moreover, elasticity correlated to walking capacity and balance tests, but not to knee extension strength.

Speed-of-sound US is an innovative US method for the assessment of tissue composition and muscle quality [101] [102]. US waves travel through different soft tissues at different speeds. US waves travel within muscle tissue with a higher speed compared to the speed of waves passing through adipose tissue [102]. Measurement of the waves’ average speed can provide information about the amount of fat tissue. Sanabria et al. [102] compared the speed of US waves passing through calf muscles between young and elderly women, using a linear high-frequency transducer. The speed of sound was significantly higher in young individuals, due to the increased amount of intermuscular and subcutaneous fat in the latter group. In addition, the speed of sound correlated to muscle function tests, showing perspective in sarcopenia diagnosis.
A disadvantage of US is the limited visualization in obese individuals that may affect the measurement [95]. US is highly operator-dependent and is influenced by the machine quality [42]. However, the main limitation is currently the lack of consensus about the muscle or muscle groups that should be evaluated, the use of simple measurement of a certain formula/index, the measuring point, and the optimal US acquisition parameters or characteristic of the muscles for the evaluation of sarcopenia [103].
The strengths and the weaknesses of the imaging methods for muscle evaluation and diagnosis of sarcopenia are summarized in [Table 1].
Conclusion
Sarcopenia and muscle atrophy are not identical processes and should not be equated. Unlike disuse atrophy, sarcopenia includes irreversible muscle changes that alter both muscle quantity and quality. The established imaging methods for muscle quantity assessment correlate to gold standard tests. However, muscle quality is probably the most important element for indirect evaluation of muscle function and diagnosis of sarcopenia in the future. Recent studies on imaging techniques that focus on different aspects of muscle quality, such as myosteatosis, myofibrosis, architectural, microstructural, and composition changes, and muscle elasticity show encouraging results. Although significant progress has been achieved, several issues regarding the imaging of muscle quality remain. The optimal methods, muscle or muscle groups that should be evaluated, measuring spots, standardized acquisition protocols, and cut-off values are either not established or not commonly accepted for most of the existing techniques. In addition, many of the previously described imaging methods of assessing muscle quantity and quality are primarily research tools and are still not validated for day-to-day practice. Future researchers should focus on overcoming these issues to provide unified, integrated characterization of sarcopenia as a disease.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Xia L, Zhao R, Wan Q. et al. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med 2020; 9: 7964-7978
- 2 Cruz-Jentoft AJ, Baeyens JP, Bauer JM. et al. European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010; 39: 412-423
- 3 Rosenberg I. Summary comments: epidemiological and methodological problems in determining nutritional status of older persons. Am J Clin Nutr 1989; 50: 1231-1233
- 4 Narici MV, Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 2010; 95: 139-159
- 5 Rozenberg D, Martelli V, Vieira L. et al. Utilization of non-invasive imaging tools for assessment of peripheral skeletal muscle size and composition in chronic lung disease: A systematic review. Respir Med 2017; 131: 125-134
- 6 Delmonico MJ, Harris TB, Visser M. et al. Health, Aging, and Body. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am J Clin Nutr 2009; 90: 1579-1585
- 7 Doherty TJ. Invited review: Aging and sarcopenia. J Appl Physiol (1985) 2003; 95: 1717-1727
- 8 Schaap LA, van Schoor NM, Lips P. et al. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J Gerontol A Biol Sci Med Sci 2018; 73: 1199-1204
- 9 Goodpaster BH, Park SW, Harris TB. et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study§#ITL#§. J Gerontol A Biol Sci Med Sci 2006; 61: 1059-1064
- 10 Cruz-Jentoft AJ, Bahat G, Bauer J. et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019; 48: 16-31
- 11 Costanzo L, De Vincentis A, Di Iorio A. et al. Impact of Low Muscle Mass and Low Muscle Strength According to EWGSOP2 and EWGSOP1 in Community-Dwelling Older People. J Gerontol A Biol Sci Med Sci 2020; 75: 1324-1330
- 12 Buchman AS, Leurgans SE, Wang T. et al. Motor function is the primary driver of the associations of sarcopenia and physical frailty with adverse health outcomes in community-dwelling older adults. PLoS One 2021; 16: e0245680
- 13 Beaudart C, Rolland Y, Cruz-Jentoft AJ. et al. Assessment of Muscle Function and Physical Performance in Daily Clinical Practice: A position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif Tissue Int 2019; 105: 1-14
- 14 McGregor RA, Cameron-Smith D, Poppitt SD. It is not just muscle mass: a review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev Healthspan 2014; 3: 9
- 15 Chiles ShafferN, Fabbri E, Ferrucci L. et al. Muscle Quality, Strength, and Lower Extremity Physical Performance in the Baltimore Longitudinal Study of Aging. J Frailty Aging 2017; 6: 183-187
- 16 Heymsfield SB, Gonzalez MC, Lu J. et al. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc 2015; 74: 355-366
- 17 Barbat-Artigas S, Rolland Y, Zamboni M. et al. How to assess functional status: a new muscle quality index. J Nutr Health Aging 2012; 16: 67-77
- 18 Correa-de-Araujo R, Harris-Love MO, Miljkovic I. et al. The Need for Standardized Assessment of Muscle Quality in Skeletal Muscle Function Deficit and Other Aging-Related Muscle Dysfunctions: A Symposium Report. Front Physiol 2017; 8: 87
- 19 Guglielmi G, Ponti F, Agostini M. et al. The role of DXA in sarcopenia. Aging Clin Exp Res 2016; 28: 1047-1060
- 20 Lee K, Shin Y, Huh J. et al. Recent Issues on Body Composition Imaging for Sarcopenia Evaluation. Korean J Radiol 2019; 20: 205-217
- 21 Messina C, Maffi G, Vitale JA. et al. Diagnostic imaging of osteoporosis and sarcopenia: a narrative review. Quant Imaging Med Surg 2018; 8: 86-99
- 22 Mettler Jr FA, Huda W, Yoshizumi TT. et al. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248: 254-263
- 23 Petak S, Barbu CG, Yu EW. et al. The Official Positions of the International Society for Clinical Densitometry: body composition analysis reporting. J Clin Densitom 2013; 16: 508-519
- 24 Baumgartner RN, Koehler KM, Gallagher D. et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998; 147: 755-763
- 25 Walowski CO, Braun W, Maisch MJ. et al. Reference Values for Skeletal Muscle Mass – Current Concepts and Methodological Considerations. Nutrients 2020; 12: 755
- 26 Lindqvist C, Brismar TB, Majeed A. et al. Assessment of muscle mass depletion in chronic liver disease: Dual-energy x-ray absorptiometry compared with computed tomography. Nutrition 2019; 61: 93-98
- 27 Tosato M, Marzetti E, Cesari M. et al. Measurement of muscle mass in sarcopenia: from imaging to biochemical markers. Aging Clin Exp Res 2017; 29: 19-27
- 28 Bredella MA, Ghomi RH, Thomas BJ. et al. Comparison of DXA and CT in the assessment of body composition in premenopausal women with obesity and anorexia nervosa. Obesity (Silver Spring) 2010; 18: 2227-2233
- 29 Cawthon PM, Peters KW, Shardell MD. et al. Cutpoints for low appendicular lean mass that identify older adults with clinically significant weakness. J Gerontol A Biol Sci Med Sci 2014; 69: 567-575
- 30 Albano D, Messina C, Vitale J. et al. Imaging of sarcopenia: old evidence and new insights. Eur Radiol 2020; 30: 2199-2208
- 31 Graffy PM, Liu J, Pickhardt PJ. et al. Deep learning-based muscle segmentation and quantification at abdominal CT: application to a longitudinal adult screening cohort for sarcopenia assessment. Br J Radiol 2019; 92: 20190327
- 32 Boutin RD, Lenchik L. Value-Added Opportunistic CT: Insights Into Osteoporosis and Sarcopenia. Am J Roentgenol 2020; 215: 582-594
- 33 Mourtzakis M, Prado CM, Lieffers JR. et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab 2008; 33: 997-1006
- 34 Yip C, Dinkel C, Mahajan A. et al. Imaging body composition in cancer patients: visceral obesity, sarcopenia and sarcopenic obesity may impact on clinical outcome. Insights Imaging 2015; 6: 489-497
- 35 Amini B, Boyle SP, Boutin RD. et al. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography: A Systematic Review. J Gerontol A Biol Sci Med Sci 2019; 74: 1671-1678
- 36 Ishida Y, Maeda K, Yamanaka Y. et al. Formula for the Cross-Sectional Area of the Muscles of the Third Lumbar Vertebra Level from the Twelfth Thoracic Vertebra Level Slice on Computed Tomography. Geriatrics (Basel) 2020; 5 (03) 47
- 37 Matsuyama R, Maeda K, Yamanaka Y. et al. Assessing skeletal muscle mass based on the cross-sectional area of muscles at the 12th thoracic vertebra level on computed tomography in patients with oral squamous cell carcinoma. Oral Oncol 2021; 113: 105126
- 38 Sanders KJC, Degens JHRJ, Dingemans AC. et al. Cross-sectional and longitudinal assessment of muscle from regular chest computed tomography scans: L1 and pectoralis muscle compared to L3 as reference in non-small cell lung cancer. Int J Chron Obstruct Pulmon Dis 2019; 14: 781-789
- 39 Swartz JE, Pothen AJ, Wegner I. et al. Feasibility of using head and neck CT imaging to assess skeletal muscle mass in head and neck cancer patients. Oral Oncol 2016; 62: 28-33
- 40 Jung AR, Roh JL, Kim JS. et al. Efficacy of head and neck computed tomography for skeletal muscle mass estimation in patients with head and neck cancer. Oral Oncol 2019; 95: 95-99
- 41 Prado CM, Lieffers JR, McCargar LJ. et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol 2008; 9: 629-635
- 42 Correa-de-Araujo R, Addison O, Miljkovic I. et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An Interdisciplinary Workshop at the National Institute on Aging. Front Physiol 2020; 11: 963
- 43 Zamboni M, Gattazzo S, Rossi AP. Myosteatosis: a relevant, yet poorly explored element of sarcopenia. Eur Geriatr Med 2019; 10: 5-6
- 44 Perkisas S, De Cock AM, Verhoeven V. et al. Intramuscular Adipose Tissue and the Functional Components of Sarcopenia in Hospitalized Geriatric Patients. Geriatrics (Basel) 2017; 2: 1
- 45 Boutin RD, Kaptuch JM, Bateni CP. et al. Influence of IV contrast administration on CT measures of muscle and bone attenuation: implications for sarcopenia and osteoporosis evaluation. Am J Roentgenol 2016; 207: 1046-1054
- 46 Ackermans LLGC, Volmer L, Wee L. et al. Deep Learning Automated Segmentation for Muscle and Adipose Tissue from Abdominal Computed Tomography in Polytrauma Patients. Sensors (Basel) 2021; 21: 2083
- 47 Paris MT, Tandon P, Heyland DK. et al. Automated body composition analysis of clinically acquired computed tomography scans using neural networks. Clin Nutr 2020; 39: 3049-3055
- 48 Baracos V, Kazemi-Bajestani SM. Clinical outcomes related to muscle mass in humans with cancer and catabolic illnesses. Int J Biochem Cell Biol 2013; 45: 2302-2308
- 49 Su H, Ruan J, Chen T. et al. CT-assessed sarcopenia is a predictive factor for both long-term and short-term outcomes in gastrointestinal oncology patients: a systematic review and meta-analysis. Cancer Imaging 2019; 19: 82
- 50 Xia W, Barazanchi AWH, MacFater WS. et al. The impact of computed tomography-assessed sarcopenia on outcomes for trauma patients – a systematic review and meta-analysis§#ITL#§. Injury 2019; 50: 1565-1576
- 51 Lee CM, Kang J. Prognostic impact of myosteatosis in patients with colorectal cancer: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 2020; 11: 1270-1282
- 52 Martin L, Gioulbasanis I, Senesse P. et al. Cancer-Associated Malnutrition and CT-Defined Sarcopenia and Myosteatosis Are Endemic in Overweight and Obese Patients. JPEN J Parenter Enteral Nutr 2020; 44: 227-238
- 53 Prado CM, Heymsfield SB. Lean tissue imaging: a new era for nutritional assessment and intervention. JPEN J Parenter Enteral Nutr 2014; 38: 940-953
- 54 Hepple RT. Muscle atrophy is not always sarcopenia. J Appl Physiol (1985) 2012; 113: 677-679
- 55 Codari M, Zanardo M, di Sabato ME. et al. MRI-Derived Biomarkers Related to Sarcopenia: A Systematic Review. J Magn Reson Imaging 2020; 51: 1117-1127
- 56 Shen W, Punyanitya M, Wang Z. et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985) 2004; 97: 2333-2338
- 57 Ogawa M, Lester R, Akima H. et al. Quantification of intermuscular and intramuscular adipose tissue using magnetic resonance imaging after neurodegenerative disorders. Neural Regen Res 2017; 12: 2100-2105
- 58 Sinelnikov A, Qu C, Fetzer DT. et al. Measurement of skeletal muscle area: Comparison of CT and MR imaging. Eur J Radiol 2016; 85: 1716-1721
- 59 Wang FZ, Sun H, Zhou J. et al Reliability and Validity of Abdominal Skeletal Muscle Area Measurement Using Magnetic Resonance Imaging. Acad Radiol 2020; 28 S1076-6332(20)30552-3.
- 60 Faron A, Sprinkart AM, Kuetting DLR. et al. Body composition analysis using CT and MRI: intra-individual intermodal comparison of muscle mass and myosteatosis. Sci Rep 2020; 10: 11765
- 61 Beer L, Bastati N, Ba-Ssalamah A. et al. MRI-defined sarcopenia predicts mortality in patients with chronic liver disease. Liver Int 2020; 40: 2797-2807
- 62 Engelke K, Museyko O, Wang L. et al. Quantitative analysis of skeletal muscle by computed tomography imaging-State of the art. J Orthop Translat 2018; 15: 91-103
- 63 Giraudo C, Cavaliere A, Lupi A. et al. Established paths and new avenues: a review of the main radiological techniques for investigating sarcopenia. Quant Imaging Med Surg 2020; 10: 1602-1613
- 64 Huber FA, Del GrandeF, Rizzo S. et al. MRI in the assessment of adipose tissues and muscle composition: how to use it. Quant Imaging Med Surg 2020; 10: 1636-1649
- 65 Schlaeger S, Inhuber S, Rohrmeier A. et al. Association of paraspinal muscle water-fat MRI-based measurements with isometric strength measurements. Eur Radiol 2019; 29: 599-608
- 66 Boesch C. Musculoskeletal spectroscopy. J Magn Reson Imaging 2007; 25: 321-338
- 67 Grimm A, Meyer H, Nickel MD. et al. A Comparison between 6-point Dixon MRI and MR Spectroscopy to Quantify Muscle Fat in the Thigh of Subjects with Sarcopenia. J Frailty Aging 2019; 8: 21-26
- 68 Hinkley JM, Coen PM. Muscle phosphorus metabolites in sarcopenia. Aging (Albany NY) 2020; 12: 15880-15881
- 69 Funai K, Summers SA, Rutter J. Reign in the membrane: How common lipids govern mitochondrial function. Curr Opin Cell Biol 2020; 63: 162-173
- 70 Hinkley JM, Cornnell HH, Standley RA. et al. Older adults with sarcopenia have distinct skeletal muscle phosphodiester, phosphocreatine, and phospholipid profiles. Aging Cell 2020; 19: e13135
- 71 Zoico E, Corzato F, Bambace C. et al. Myosteatosis and myofibrosis: relationship with aging, inflammation and insulin resistance. Arch Gerontol Geriatr 2013; 57: 411-416
- 72 Boutin RD, Yao L, Canter RJ. et al. Sarcopenia: Current Concepts and Imaging Implications. Am J Roentgenol 2015; 205: W255-266
- 73 Sinha U, Malis V, Csapo R. et al. Age-related differences in strain rate tensor of the medial gastrocnemius muscle during passive plantarflexion and active isometric contraction using velocity encoded MR imaging: potential index of lateral force transmission. Magn Reson Med 2015; 73: 1852-1863
- 74 Azzabou N, Hogrel JY, Carlier PG. NMR based biomarkers to study age-related changes in the human quadriceps. Exp Gerontol 2015; 70: 54-60
- 75 Oudeman J, Nederveen AJ, Strijkers GJ. et al. Techniques and applications of skeletal muscle diffusion tensor imaging: A review. J Magn Reson Imaging 2016; 43: 773-788
- 76 Galbán CJ, Maderwald S, Stock F. et al. Age-related changes in skeletal muscle as detected by diffusion tensor magnetic resonance imaging. J Gerontol A Biol Sci Med Sci 2007; 62: 453-458
- 77 Farrow M, Biglands J, Tanner SF. et al. The effect of ageing on skeletal muscle as assessed by quantitative MR imaging: an association with frailty and muscle strength. Aging Clin Exp Res 2021; 33: 291-301
- 78 Erlandson MC, Lorbergs AL, Mathur S. et al. Muscle analysis using pQCT, DXA and MRI. Eur J Radiol 2016; 85: 1505-1511
- 79 Abe T, Thiebaud RS, Loenneke JP. et al. Prediction and validation of DXA-derived appendicular lean soft tissue mass by ultrasound in older adults. Age (Dordr) 2015; 37: 114
- 80 Hida T, Ando K, Kobayashi K. et al. <Editors' Choice> Ultrasound measurement of thigh muscle thickness for assessment of sarcopenia. Nagoya J Med Sci 2018; 80: 519-527
- 81 Souza VA, Oliveira D, Cupolilo EN. et al. Rectus femoris muscle mass evaluation by ultrasound: facilitating sarcopenia diagnosis in pre-dialysis chronic kidney disease stages. Clinics (Sao Paulo) 2018; 73: e392
- 82 Sanada K, Kearns CF, Midorikawa T. et al. Prediction and validation of total and regional skeletal muscle mass by ultrasound in Japanese adults. Eur J Appl Physiol 2006; 96: 24-31
- 83 Ivanoski S, Vasilevska Nikodinovska V. Future Ultrasound Biomarkers for Sarcopenia: Elastography, Contrast-Enhanced Ultrasound, and Speed of Sound Ultrasound Imaging. Semin Musculoskelet Radiol 2020; 24: 194-200
- 84 Akagi R, Suzuki M, Kawaguchi E. et al. Muscle size-strength relationship including ultrasonographic echo intensity and voluntary activation level of a muscle group. Arch Gerontol Geriatr 2018; 75: 185-190
- 85 Janssen I, Heymsfield SB, Wang ZM. et al. Skeletal muscle mass and distribution in 468 men and women aged 18-88 yr. J Appl Physiol (1985) 2000; 89: 81-88
- 86 Minetto MA, Caresio C, Menapace T. et al. Ultrasound-Based Detection of Low Muscle Mass for Diagnosis of Sarcopenia in Older Adults. PM R 2016; 8: 453-462
- 87 Narici MV, Franchi MV, Maganaris CN. Muscle structural assembly and functional consequences. J Exp Biol 2015; 219: 276-284
- 88 Ward SR, Eng CM, Smallwood LH. et al. Are current measurements of lower extremity muscle architecture accurate?. Clin Orthop Relat Res 2009; 467: 1074-1082
- 89 Roberts TJ, Eng CM, Sleboda DA. et al. The Multi-Scale, Three-Dimensional Nature of Skeletal Muscle Contraction. Physiology (Bethesda) 2019; 34: 402-408
- 90 Mirón Mombiela R, Vucetic J, Rossi F. et al. Ultrasound Biomarkers for Sarcopenia: What Can We Tell So Far?. Semin Musculoskelet Radiol 2020; 24: 181-193
- 91 Narici MV, Maganaris CN, Reeves ND. et al. Effect of aging on human muscle architecture. J Appl Physiol (1985) 2003; 95: 2229-2234
- 92 Ticinesi A, Meschi T, Narici MV. et al. Muscle Ultrasound and Sarcopenia in Older Individuals: A Clinical Perspective. J Am Med Dir Assoc 2017; 18: 290-300
- 93 Mirón Mombiela R, Facal de Castro F, Moreno P. et al. Ultrasonic Echo Intensity as a New Noninvasive In Vivo Biomarker of Frailty. J Am Geriatr Soc 2017; 65: 2685-2690
- 94 Watanabe Y, Yamada Y, Fukumoto Y. et al. Echo intensity obtained from ultrasonography images reflecting muscle strength in elderly men. Clin Interv Aging 2013; 8: 993-998
- 95 Stringer HJ, Wilson D. The Role of Ultrasound as a Diagnostic Tool for Sarcopenia. J Frailty Aging 2018; 7: 258-261
- 96 Akima H, Hioki M, Yoshiko A. et al. Intramuscular adipose tissue determined by T1-weighted MRI at 3T primarily reflects extramyocellular lipids. Magn Reson Imaging 2016; 34: 397-403
- 97 Harris-Love MO, Avila NA, Adams B. et al. The Comparative Associations of Ultrasound and Computed Tomography Estimates of Muscle Quality with Physical Performance and Metabolic Parameters in Older Men. J Clin Med 2018; 7: 340
- 98 Isaka M, Sugimoto K, Yasunobe Y. et al. The Usefulness of an Alternative Diagnostic Method for Sarcopenia Using Thickness and Echo Intensity of Lower Leg Muscles in Older Males. J Am Med Dir Assoc 2019; 20: 1185.e1-1185.e8
- 99 Bastijns S, De Cock AM, Vandewoude M. et al. Usability and Pitfalls of Shear-Wave Elastography for Evaluation of Muscle Quality and Its Potenzial in Assessing Sarcopenia: A Review. Ultrasound Med Biol 2020; 46: 2891-2907
- 100 Saito A, Wakasa M, Kimoto M. et al. Age-related changes in muscle elasticity and thickness of the lower extremities are associated with physical functions among community-dwelling older women. Geriatr Gerontol Int 2019; 19: 61-65
- 101 Sanabria SJ, Martini K, Freystätter G. et al. Speed of sound ultrasound: a pilot study on a novel technique to identify sarcopenia in seniors. Eur Radiol 2019; 29: 3-12
- 102 Sanabria SJ, Goksel O, Martini K. et al. Breast-density assessment with hand-held ultrasound: A novel biomarker to assess breast cancer risk and to tailor screening?. Eur Radiol 2018; 28: 3165-3175
- 103 Perkisas S, Baudry S, Bauer J. et al. Application of ultrasound for muscle assessment in sarcopenia: towards standardized measurements. Eur Geriatr Med 2018; 9: 739-757
Correspondence
Publication History
Received: 28 November 2022
Accepted: 06 March 2023
Article published online:
09 May 2023
© 2023. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Xia L, Zhao R, Wan Q. et al. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med 2020; 9: 7964-7978
- 2 Cruz-Jentoft AJ, Baeyens JP, Bauer JM. et al. European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010; 39: 412-423
- 3 Rosenberg I. Summary comments: epidemiological and methodological problems in determining nutritional status of older persons. Am J Clin Nutr 1989; 50: 1231-1233
- 4 Narici MV, Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 2010; 95: 139-159
- 5 Rozenberg D, Martelli V, Vieira L. et al. Utilization of non-invasive imaging tools for assessment of peripheral skeletal muscle size and composition in chronic lung disease: A systematic review. Respir Med 2017; 131: 125-134
- 6 Delmonico MJ, Harris TB, Visser M. et al. Health, Aging, and Body. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am J Clin Nutr 2009; 90: 1579-1585
- 7 Doherty TJ. Invited review: Aging and sarcopenia. J Appl Physiol (1985) 2003; 95: 1717-1727
- 8 Schaap LA, van Schoor NM, Lips P. et al. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J Gerontol A Biol Sci Med Sci 2018; 73: 1199-1204
- 9 Goodpaster BH, Park SW, Harris TB. et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study§#ITL#§. J Gerontol A Biol Sci Med Sci 2006; 61: 1059-1064
- 10 Cruz-Jentoft AJ, Bahat G, Bauer J. et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019; 48: 16-31
- 11 Costanzo L, De Vincentis A, Di Iorio A. et al. Impact of Low Muscle Mass and Low Muscle Strength According to EWGSOP2 and EWGSOP1 in Community-Dwelling Older People. J Gerontol A Biol Sci Med Sci 2020; 75: 1324-1330
- 12 Buchman AS, Leurgans SE, Wang T. et al. Motor function is the primary driver of the associations of sarcopenia and physical frailty with adverse health outcomes in community-dwelling older adults. PLoS One 2021; 16: e0245680
- 13 Beaudart C, Rolland Y, Cruz-Jentoft AJ. et al. Assessment of Muscle Function and Physical Performance in Daily Clinical Practice: A position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif Tissue Int 2019; 105: 1-14
- 14 McGregor RA, Cameron-Smith D, Poppitt SD. It is not just muscle mass: a review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev Healthspan 2014; 3: 9
- 15 Chiles ShafferN, Fabbri E, Ferrucci L. et al. Muscle Quality, Strength, and Lower Extremity Physical Performance in the Baltimore Longitudinal Study of Aging. J Frailty Aging 2017; 6: 183-187
- 16 Heymsfield SB, Gonzalez MC, Lu J. et al. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc 2015; 74: 355-366
- 17 Barbat-Artigas S, Rolland Y, Zamboni M. et al. How to assess functional status: a new muscle quality index. J Nutr Health Aging 2012; 16: 67-77
- 18 Correa-de-Araujo R, Harris-Love MO, Miljkovic I. et al. The Need for Standardized Assessment of Muscle Quality in Skeletal Muscle Function Deficit and Other Aging-Related Muscle Dysfunctions: A Symposium Report. Front Physiol 2017; 8: 87
- 19 Guglielmi G, Ponti F, Agostini M. et al. The role of DXA in sarcopenia. Aging Clin Exp Res 2016; 28: 1047-1060
- 20 Lee K, Shin Y, Huh J. et al. Recent Issues on Body Composition Imaging for Sarcopenia Evaluation. Korean J Radiol 2019; 20: 205-217
- 21 Messina C, Maffi G, Vitale JA. et al. Diagnostic imaging of osteoporosis and sarcopenia: a narrative review. Quant Imaging Med Surg 2018; 8: 86-99
- 22 Mettler Jr FA, Huda W, Yoshizumi TT. et al. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248: 254-263
- 23 Petak S, Barbu CG, Yu EW. et al. The Official Positions of the International Society for Clinical Densitometry: body composition analysis reporting. J Clin Densitom 2013; 16: 508-519
- 24 Baumgartner RN, Koehler KM, Gallagher D. et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998; 147: 755-763
- 25 Walowski CO, Braun W, Maisch MJ. et al. Reference Values for Skeletal Muscle Mass – Current Concepts and Methodological Considerations. Nutrients 2020; 12: 755
- 26 Lindqvist C, Brismar TB, Majeed A. et al. Assessment of muscle mass depletion in chronic liver disease: Dual-energy x-ray absorptiometry compared with computed tomography. Nutrition 2019; 61: 93-98
- 27 Tosato M, Marzetti E, Cesari M. et al. Measurement of muscle mass in sarcopenia: from imaging to biochemical markers. Aging Clin Exp Res 2017; 29: 19-27
- 28 Bredella MA, Ghomi RH, Thomas BJ. et al. Comparison of DXA and CT in the assessment of body composition in premenopausal women with obesity and anorexia nervosa. Obesity (Silver Spring) 2010; 18: 2227-2233
- 29 Cawthon PM, Peters KW, Shardell MD. et al. Cutpoints for low appendicular lean mass that identify older adults with clinically significant weakness. J Gerontol A Biol Sci Med Sci 2014; 69: 567-575
- 30 Albano D, Messina C, Vitale J. et al. Imaging of sarcopenia: old evidence and new insights. Eur Radiol 2020; 30: 2199-2208
- 31 Graffy PM, Liu J, Pickhardt PJ. et al. Deep learning-based muscle segmentation and quantification at abdominal CT: application to a longitudinal adult screening cohort for sarcopenia assessment. Br J Radiol 2019; 92: 20190327
- 32 Boutin RD, Lenchik L. Value-Added Opportunistic CT: Insights Into Osteoporosis and Sarcopenia. Am J Roentgenol 2020; 215: 582-594
- 33 Mourtzakis M, Prado CM, Lieffers JR. et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab 2008; 33: 997-1006
- 34 Yip C, Dinkel C, Mahajan A. et al. Imaging body composition in cancer patients: visceral obesity, sarcopenia and sarcopenic obesity may impact on clinical outcome. Insights Imaging 2015; 6: 489-497
- 35 Amini B, Boyle SP, Boutin RD. et al. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography: A Systematic Review. J Gerontol A Biol Sci Med Sci 2019; 74: 1671-1678
- 36 Ishida Y, Maeda K, Yamanaka Y. et al. Formula for the Cross-Sectional Area of the Muscles of the Third Lumbar Vertebra Level from the Twelfth Thoracic Vertebra Level Slice on Computed Tomography. Geriatrics (Basel) 2020; 5 (03) 47
- 37 Matsuyama R, Maeda K, Yamanaka Y. et al. Assessing skeletal muscle mass based on the cross-sectional area of muscles at the 12th thoracic vertebra level on computed tomography in patients with oral squamous cell carcinoma. Oral Oncol 2021; 113: 105126
- 38 Sanders KJC, Degens JHRJ, Dingemans AC. et al. Cross-sectional and longitudinal assessment of muscle from regular chest computed tomography scans: L1 and pectoralis muscle compared to L3 as reference in non-small cell lung cancer. Int J Chron Obstruct Pulmon Dis 2019; 14: 781-789
- 39 Swartz JE, Pothen AJ, Wegner I. et al. Feasibility of using head and neck CT imaging to assess skeletal muscle mass in head and neck cancer patients. Oral Oncol 2016; 62: 28-33
- 40 Jung AR, Roh JL, Kim JS. et al. Efficacy of head and neck computed tomography for skeletal muscle mass estimation in patients with head and neck cancer. Oral Oncol 2019; 95: 95-99
- 41 Prado CM, Lieffers JR, McCargar LJ. et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol 2008; 9: 629-635
- 42 Correa-de-Araujo R, Addison O, Miljkovic I. et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An Interdisciplinary Workshop at the National Institute on Aging. Front Physiol 2020; 11: 963
- 43 Zamboni M, Gattazzo S, Rossi AP. Myosteatosis: a relevant, yet poorly explored element of sarcopenia. Eur Geriatr Med 2019; 10: 5-6
- 44 Perkisas S, De Cock AM, Verhoeven V. et al. Intramuscular Adipose Tissue and the Functional Components of Sarcopenia in Hospitalized Geriatric Patients. Geriatrics (Basel) 2017; 2: 1
- 45 Boutin RD, Kaptuch JM, Bateni CP. et al. Influence of IV contrast administration on CT measures of muscle and bone attenuation: implications for sarcopenia and osteoporosis evaluation. Am J Roentgenol 2016; 207: 1046-1054
- 46 Ackermans LLGC, Volmer L, Wee L. et al. Deep Learning Automated Segmentation for Muscle and Adipose Tissue from Abdominal Computed Tomography in Polytrauma Patients. Sensors (Basel) 2021; 21: 2083
- 47 Paris MT, Tandon P, Heyland DK. et al. Automated body composition analysis of clinically acquired computed tomography scans using neural networks. Clin Nutr 2020; 39: 3049-3055
- 48 Baracos V, Kazemi-Bajestani SM. Clinical outcomes related to muscle mass in humans with cancer and catabolic illnesses. Int J Biochem Cell Biol 2013; 45: 2302-2308
- 49 Su H, Ruan J, Chen T. et al. CT-assessed sarcopenia is a predictive factor for both long-term and short-term outcomes in gastrointestinal oncology patients: a systematic review and meta-analysis. Cancer Imaging 2019; 19: 82
- 50 Xia W, Barazanchi AWH, MacFater WS. et al. The impact of computed tomography-assessed sarcopenia on outcomes for trauma patients – a systematic review and meta-analysis§#ITL#§. Injury 2019; 50: 1565-1576
- 51 Lee CM, Kang J. Prognostic impact of myosteatosis in patients with colorectal cancer: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 2020; 11: 1270-1282
- 52 Martin L, Gioulbasanis I, Senesse P. et al. Cancer-Associated Malnutrition and CT-Defined Sarcopenia and Myosteatosis Are Endemic in Overweight and Obese Patients. JPEN J Parenter Enteral Nutr 2020; 44: 227-238
- 53 Prado CM, Heymsfield SB. Lean tissue imaging: a new era for nutritional assessment and intervention. JPEN J Parenter Enteral Nutr 2014; 38: 940-953
- 54 Hepple RT. Muscle atrophy is not always sarcopenia. J Appl Physiol (1985) 2012; 113: 677-679
- 55 Codari M, Zanardo M, di Sabato ME. et al. MRI-Derived Biomarkers Related to Sarcopenia: A Systematic Review. J Magn Reson Imaging 2020; 51: 1117-1127
- 56 Shen W, Punyanitya M, Wang Z. et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985) 2004; 97: 2333-2338
- 57 Ogawa M, Lester R, Akima H. et al. Quantification of intermuscular and intramuscular adipose tissue using magnetic resonance imaging after neurodegenerative disorders. Neural Regen Res 2017; 12: 2100-2105
- 58 Sinelnikov A, Qu C, Fetzer DT. et al. Measurement of skeletal muscle area: Comparison of CT and MR imaging. Eur J Radiol 2016; 85: 1716-1721
- 59 Wang FZ, Sun H, Zhou J. et al Reliability and Validity of Abdominal Skeletal Muscle Area Measurement Using Magnetic Resonance Imaging. Acad Radiol 2020; 28 S1076-6332(20)30552-3.
- 60 Faron A, Sprinkart AM, Kuetting DLR. et al. Body composition analysis using CT and MRI: intra-individual intermodal comparison of muscle mass and myosteatosis. Sci Rep 2020; 10: 11765
- 61 Beer L, Bastati N, Ba-Ssalamah A. et al. MRI-defined sarcopenia predicts mortality in patients with chronic liver disease. Liver Int 2020; 40: 2797-2807
- 62 Engelke K, Museyko O, Wang L. et al. Quantitative analysis of skeletal muscle by computed tomography imaging-State of the art. J Orthop Translat 2018; 15: 91-103
- 63 Giraudo C, Cavaliere A, Lupi A. et al. Established paths and new avenues: a review of the main radiological techniques for investigating sarcopenia. Quant Imaging Med Surg 2020; 10: 1602-1613
- 64 Huber FA, Del GrandeF, Rizzo S. et al. MRI in the assessment of adipose tissues and muscle composition: how to use it. Quant Imaging Med Surg 2020; 10: 1636-1649
- 65 Schlaeger S, Inhuber S, Rohrmeier A. et al. Association of paraspinal muscle water-fat MRI-based measurements with isometric strength measurements. Eur Radiol 2019; 29: 599-608
- 66 Boesch C. Musculoskeletal spectroscopy. J Magn Reson Imaging 2007; 25: 321-338
- 67 Grimm A, Meyer H, Nickel MD. et al. A Comparison between 6-point Dixon MRI and MR Spectroscopy to Quantify Muscle Fat in the Thigh of Subjects with Sarcopenia. J Frailty Aging 2019; 8: 21-26
- 68 Hinkley JM, Coen PM. Muscle phosphorus metabolites in sarcopenia. Aging (Albany NY) 2020; 12: 15880-15881
- 69 Funai K, Summers SA, Rutter J. Reign in the membrane: How common lipids govern mitochondrial function. Curr Opin Cell Biol 2020; 63: 162-173
- 70 Hinkley JM, Cornnell HH, Standley RA. et al. Older adults with sarcopenia have distinct skeletal muscle phosphodiester, phosphocreatine, and phospholipid profiles. Aging Cell 2020; 19: e13135
- 71 Zoico E, Corzato F, Bambace C. et al. Myosteatosis and myofibrosis: relationship with aging, inflammation and insulin resistance. Arch Gerontol Geriatr 2013; 57: 411-416
- 72 Boutin RD, Yao L, Canter RJ. et al. Sarcopenia: Current Concepts and Imaging Implications. Am J Roentgenol 2015; 205: W255-266
- 73 Sinha U, Malis V, Csapo R. et al. Age-related differences in strain rate tensor of the medial gastrocnemius muscle during passive plantarflexion and active isometric contraction using velocity encoded MR imaging: potential index of lateral force transmission. Magn Reson Med 2015; 73: 1852-1863
- 74 Azzabou N, Hogrel JY, Carlier PG. NMR based biomarkers to study age-related changes in the human quadriceps. Exp Gerontol 2015; 70: 54-60
- 75 Oudeman J, Nederveen AJ, Strijkers GJ. et al. Techniques and applications of skeletal muscle diffusion tensor imaging: A review. J Magn Reson Imaging 2016; 43: 773-788
- 76 Galbán CJ, Maderwald S, Stock F. et al. Age-related changes in skeletal muscle as detected by diffusion tensor magnetic resonance imaging. J Gerontol A Biol Sci Med Sci 2007; 62: 453-458
- 77 Farrow M, Biglands J, Tanner SF. et al. The effect of ageing on skeletal muscle as assessed by quantitative MR imaging: an association with frailty and muscle strength. Aging Clin Exp Res 2021; 33: 291-301
- 78 Erlandson MC, Lorbergs AL, Mathur S. et al. Muscle analysis using pQCT, DXA and MRI. Eur J Radiol 2016; 85: 1505-1511
- 79 Abe T, Thiebaud RS, Loenneke JP. et al. Prediction and validation of DXA-derived appendicular lean soft tissue mass by ultrasound in older adults. Age (Dordr) 2015; 37: 114
- 80 Hida T, Ando K, Kobayashi K. et al. <Editors' Choice> Ultrasound measurement of thigh muscle thickness for assessment of sarcopenia. Nagoya J Med Sci 2018; 80: 519-527
- 81 Souza VA, Oliveira D, Cupolilo EN. et al. Rectus femoris muscle mass evaluation by ultrasound: facilitating sarcopenia diagnosis in pre-dialysis chronic kidney disease stages. Clinics (Sao Paulo) 2018; 73: e392
- 82 Sanada K, Kearns CF, Midorikawa T. et al. Prediction and validation of total and regional skeletal muscle mass by ultrasound in Japanese adults. Eur J Appl Physiol 2006; 96: 24-31
- 83 Ivanoski S, Vasilevska Nikodinovska V. Future Ultrasound Biomarkers for Sarcopenia: Elastography, Contrast-Enhanced Ultrasound, and Speed of Sound Ultrasound Imaging. Semin Musculoskelet Radiol 2020; 24: 194-200
- 84 Akagi R, Suzuki M, Kawaguchi E. et al. Muscle size-strength relationship including ultrasonographic echo intensity and voluntary activation level of a muscle group. Arch Gerontol Geriatr 2018; 75: 185-190
- 85 Janssen I, Heymsfield SB, Wang ZM. et al. Skeletal muscle mass and distribution in 468 men and women aged 18-88 yr. J Appl Physiol (1985) 2000; 89: 81-88
- 86 Minetto MA, Caresio C, Menapace T. et al. Ultrasound-Based Detection of Low Muscle Mass for Diagnosis of Sarcopenia in Older Adults. PM R 2016; 8: 453-462
- 87 Narici MV, Franchi MV, Maganaris CN. Muscle structural assembly and functional consequences. J Exp Biol 2015; 219: 276-284
- 88 Ward SR, Eng CM, Smallwood LH. et al. Are current measurements of lower extremity muscle architecture accurate?. Clin Orthop Relat Res 2009; 467: 1074-1082
- 89 Roberts TJ, Eng CM, Sleboda DA. et al. The Multi-Scale, Three-Dimensional Nature of Skeletal Muscle Contraction. Physiology (Bethesda) 2019; 34: 402-408
- 90 Mirón Mombiela R, Vucetic J, Rossi F. et al. Ultrasound Biomarkers for Sarcopenia: What Can We Tell So Far?. Semin Musculoskelet Radiol 2020; 24: 181-193
- 91 Narici MV, Maganaris CN, Reeves ND. et al. Effect of aging on human muscle architecture. J Appl Physiol (1985) 2003; 95: 2229-2234
- 92 Ticinesi A, Meschi T, Narici MV. et al. Muscle Ultrasound and Sarcopenia in Older Individuals: A Clinical Perspective. J Am Med Dir Assoc 2017; 18: 290-300
- 93 Mirón Mombiela R, Facal de Castro F, Moreno P. et al. Ultrasonic Echo Intensity as a New Noninvasive In Vivo Biomarker of Frailty. J Am Geriatr Soc 2017; 65: 2685-2690
- 94 Watanabe Y, Yamada Y, Fukumoto Y. et al. Echo intensity obtained from ultrasonography images reflecting muscle strength in elderly men. Clin Interv Aging 2013; 8: 993-998
- 95 Stringer HJ, Wilson D. The Role of Ultrasound as a Diagnostic Tool for Sarcopenia. J Frailty Aging 2018; 7: 258-261
- 96 Akima H, Hioki M, Yoshiko A. et al. Intramuscular adipose tissue determined by T1-weighted MRI at 3T primarily reflects extramyocellular lipids. Magn Reson Imaging 2016; 34: 397-403
- 97 Harris-Love MO, Avila NA, Adams B. et al. The Comparative Associations of Ultrasound and Computed Tomography Estimates of Muscle Quality with Physical Performance and Metabolic Parameters in Older Men. J Clin Med 2018; 7: 340
- 98 Isaka M, Sugimoto K, Yasunobe Y. et al. The Usefulness of an Alternative Diagnostic Method for Sarcopenia Using Thickness and Echo Intensity of Lower Leg Muscles in Older Males. J Am Med Dir Assoc 2019; 20: 1185.e1-1185.e8
- 99 Bastijns S, De Cock AM, Vandewoude M. et al. Usability and Pitfalls of Shear-Wave Elastography for Evaluation of Muscle Quality and Its Potenzial in Assessing Sarcopenia: A Review. Ultrasound Med Biol 2020; 46: 2891-2907
- 100 Saito A, Wakasa M, Kimoto M. et al. Age-related changes in muscle elasticity and thickness of the lower extremities are associated with physical functions among community-dwelling older women. Geriatr Gerontol Int 2019; 19: 61-65
- 101 Sanabria SJ, Martini K, Freystätter G. et al. Speed of sound ultrasound: a pilot study on a novel technique to identify sarcopenia in seniors. Eur Radiol 2019; 29: 3-12
- 102 Sanabria SJ, Goksel O, Martini K. et al. Breast-density assessment with hand-held ultrasound: A novel biomarker to assess breast cancer risk and to tailor screening?. Eur Radiol 2018; 28: 3165-3175
- 103 Perkisas S, Baudry S, Bauer J. et al. Application of ultrasound for muscle assessment in sarcopenia: towards standardized measurements. Eur Geriatr Med 2018; 9: 739-757