

Subscribe to RSS
DOI: 10.1055/a-1945-9063
Use of texture and color enhancement imaging to identify the pancreatic duct orifice in a patient with a pancreaticojejunal anastomotic stricture
Authors

An endoscopic approach to pancreaticojejunal anastomotic stricture (PJAS) using a balloon enteroscope in patients who have undergone pancreaticoduodenectomy is challenging [1] [2] [3]. Identification of the pancreatic duct orifice is often difficult because of complete PJAS. Herein, we report the case of a patient with a PJAS in whom a texture and color enhancement imaging (TXI)-equipped new-generation endoscopy system (EVIS X1; Olympus Medical Systems, Japan) [4] was used, which facilitated identification of the pancreatic duct orifice.
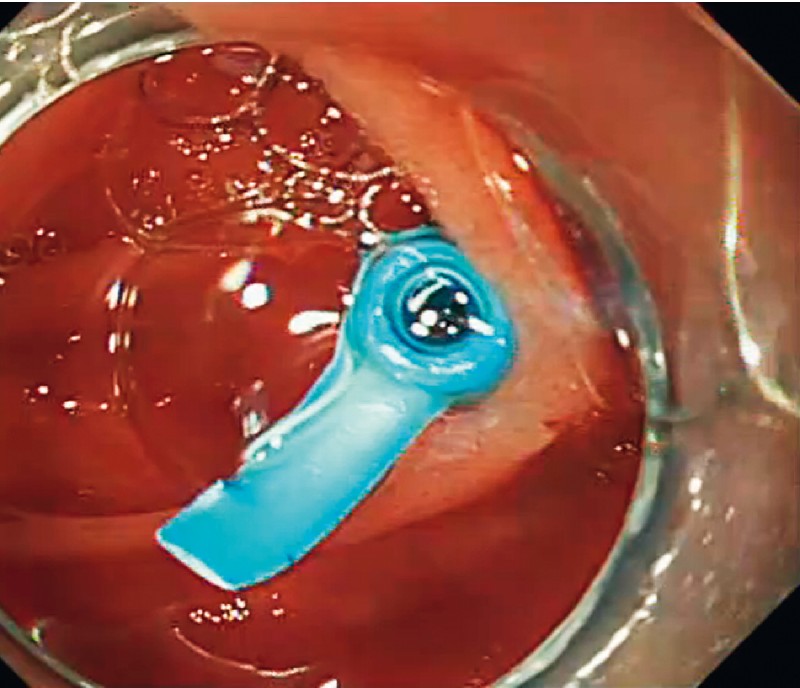
A 72-year-old woman with recurrent pancreatitis was referred to our facility. She had undergone pancreaticoduodenectomy (Child’s reconstruction) because of an intraductal papillary mucinous carcinoma. Computed tomography (CT) imaging revealed pancreatic duct dilatation and a pancreatic duct stone ([Fig. 1]). Therefore, endoscopic retrograde cholangiopancreatography (ERCP) was performed using a short-type single-balloon enteroscope (SIF-H290; Olympus Medical Systems, Tokyo, Japan) with a working length of 152 cm and a working channel of 3.2 mm in diameter [3] ([Video 1]). After reaching the site of the pancreaticojejunal anastomosis, we tried to locate the orifice of the pancreatic duct; however, it was unclear on white-light imaging (WLI) because of the PJAS ([Fig. 2 a]). Therefore, we applied TXI, which resulted in the orifice of the pancreatic duct becoming clearer ([Fig. 2 b]). Pancreatic duct cannulation could then be performed under TXI. Pancreatography confirmed pancreatic duct dilatation and a pancreatic duct stone ([Fig. 3]). A pancreatic duct stent was placed, which resulted in resolution of the patient’s pancreatitis ([Fig. 4]).

Video 1 Successful identification of the orifice of the pancreatic duct using texture and color enhancement imaging in a patient with a pancreaticojejunal anastomotic stricture.


TXI is an imaging technique that optimizes three mucosal surface elements: structure, color, and brightness; it contributes to the improved observation of lesions [4]. TXI has also been reported to facilitate transpapillary biliary cannulation [5]. In this case, TXI was extremely useful in the identification of the orifice of the pancreatic duct in a patient with PJAS. TXI could improve the success rate of ERCP using balloon enteroscopy in patients with a PJAS.
Endoscopy_UCTN_Code_CCL_1AZ_2AI
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online. Processing charges apply (currently EUR
375), discounts and wavers acc. to HINARI are available.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
-
References
- 1 Yane K, Katanuma A, Maguchi H. et al. Short-type single balloon enteroscope assisted ERCP in postsurgical altered anatomy: Potential factors affecting procedural failure. Endoscopy 2017; 49: 69-74
- 2 Kogure H, Sato T, Nakai Y. et al. Endoscopic management of pancreatic diseases in patients with surgically altered anatomy: clinical outcomes of combination of double-balloon endoscopy- and endoscopic ultrasound-guided interventions. Dig Endosc 2021; 33: 441-450
- 3 Tanisaka Y, Ryozawa S, Itoi T. et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy-assisted ERCP for altered anatomy: a multicenter cohort in Japan. Gastrointest Endosc 2022; 95: 310-318.e1
- 4 Sato T. TXI: texture and color enhancement imaging for endoscopic image enhancement. J Healthc Eng 2021;
- 5 Toyonaga H, Kin T, Hayashi T. et al. The application of texture and color enhancement imaging in transpapillary biliary cannulation. Endoscopy 2022;
Corresponding author
Publication History
Article published online:
10 October 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Yane K, Katanuma A, Maguchi H. et al. Short-type single balloon enteroscope assisted ERCP in postsurgical altered anatomy: Potential factors affecting procedural failure. Endoscopy 2017; 49: 69-74
- 2 Kogure H, Sato T, Nakai Y. et al. Endoscopic management of pancreatic diseases in patients with surgically altered anatomy: clinical outcomes of combination of double-balloon endoscopy- and endoscopic ultrasound-guided interventions. Dig Endosc 2021; 33: 441-450
- 3 Tanisaka Y, Ryozawa S, Itoi T. et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy-assisted ERCP for altered anatomy: a multicenter cohort in Japan. Gastrointest Endosc 2022; 95: 310-318.e1
- 4 Sato T. TXI: texture and color enhancement imaging for endoscopic image enhancement. J Healthc Eng 2021;
- 5 Toyonaga H, Kin T, Hayashi T. et al. The application of texture and color enhancement imaging in transpapillary biliary cannulation. Endoscopy 2022;