

Subscribe to RSS
DOI: 10.1055/a-1934-9808
Intrastone tunneling endoscopic lithotripsy technique for the treatment of Bouveret syndrome
Authors

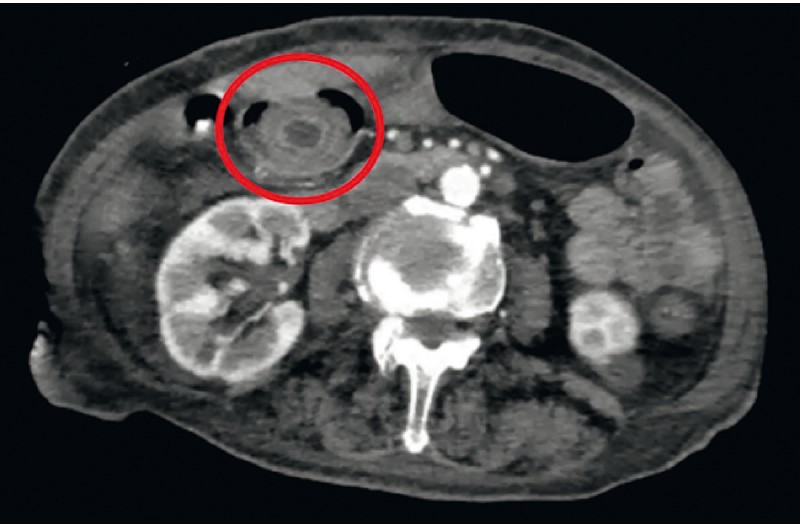
An 89-year-old woman presented with acute abdominal pain and vomiting. Computed tomography revealed a gas-filled gallbladder and a 38 × 29 mm gallstone inside the duodenal bulb, compatible with Bouveret syndrome ([Fig. 1]). After multidisciplinary discussion, endoscopic treatment was pursued ([Video 1]).
Video 1 Multistep approach using a triangle tip knife to expose the gallstone inner core was followed by electrohydraulic lithotripsy, which achieved complete stone fragmentation in a case of Bouveret syndrome.
Upper endoscopy confirmed a gallstone impacted in the duodenal bulb ([Fig. 2]). Initial removal attempt with snare and lithotripsy extraction basket was unsuccessful. Subsequent attempt at gallstone fragmentation with argon plasma coagulation was ineffective. After team discussion, a triangle tip (TT) electrosurgical knife, with spray coagulation (effect 3, 60 watts), was used, creating a tunnel to the gallstone inner core ([Fig. 3]). Due to time limitation the procedure was interrupted.


A second upper endoscopy was performed the next day. Tunnel widening, using the TT knife, further exposed the inner core. Electrohydraulic lithotripsy of the inner core was then performed, after water instillation, resulting in complete stone fragmentation ([Fig. 4]). The fragments were then removed using a net basket. Final inspection revealed superficial ulceration of the pylorus and anterosuperior wall of the bulb ([Fig. 5]). No fistulous orifice was identified. The combined time of the two procedures was 120 minutes. The patient needed no further treatment and remains well.


Gallstones have a hard inner core and soft outer shell [1]. From our experience, electrohydraulic lithotripsy is less successful in achieving fragmentation of the soft outer shell of large gallstones, making it a laborious procedure [2]. Despite previous reports of use of an electrosurgical endoscopy knife for the endoscopic treatment of bezoars [3], to our knowledge, this is the first report of its use in the management of Bouveret syndrome. In our case, the use of the TT knife allowed access to the inner core of the gallstone, which was subsequently fragmented using electrohydraulic lithotripsy. This multistep approach should be considered for large gallstones.
Endoscopy_UCTN_Code_CCL_1AZ_2AN
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online. Processing charges apply (currently EUR
375), discounts and wavers acc. to HINARI are available.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
Competing Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Futai R, Iemoto T, Inoue Y. et al. Successful treatment of Bouveret syndrome by electrohydraulic lithotripsy and double balloon endoscopy. Am J Case Rep 2019; 20: 1320-1324
- 2 Rafael MA, Figueiredo L, Horta D. et al. Treatment of Bouveret syndrome with electrohydraulic lithotripsy. Clin Endosc 2020; 53: 241-242
- 3 Maehata T, Kiyokawa H, Nakahara K. et al. Successfully combined therapy of Coca-Cola and endoscopic treatment for a giant diospyrobezoar in the duodenum using the electrosurgical endo-knife and ileus tube. VideoGIE 2021; 6: 475-477
Corresponding author
Publication History
Article published online:
14 October 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Futai R, Iemoto T, Inoue Y. et al. Successful treatment of Bouveret syndrome by electrohydraulic lithotripsy and double balloon endoscopy. Am J Case Rep 2019; 20: 1320-1324
- 2 Rafael MA, Figueiredo L, Horta D. et al. Treatment of Bouveret syndrome with electrohydraulic lithotripsy. Clin Endosc 2020; 53: 241-242
- 3 Maehata T, Kiyokawa H, Nakahara K. et al. Successfully combined therapy of Coca-Cola and endoscopic treatment for a giant diospyrobezoar in the duodenum using the electrosurgical endo-knife and ileus tube. VideoGIE 2021; 6: 475-477