

Subscribe to RSS
DOI: 10.1055/a-1718-4182
CT Planning prior to Transcatheter Mitral Valve Replacement (TMVR)
Article in several languages: English | deutschAuthors

Abstract
Background Transcatheter mitral valve replacement (TMVR) is a treatment option for patients with therapy refractory high-grade mitral valve regurgitation and a high perioperative risk.
During TMVR, the mitral annulus cannot be visualized directly. Therefore, comprehensive pre-interventional planning and a precise visualization of the patient’s specific mitral valve anatomy, outflow tract anatomy and projected anchoring of the device are necessary.
Aim of this review-article is, to assess the role of pre-procedural computed tomography (CT) for TMVR-planning
Methods Screening and evaluation of relevant guidelines (European Society of Cardiology [ESC], American Heart Association [AHA/ACC]), meta-analyses and original research using the search terms “TVMR” or “TMVI” and “CT”. In addition to this, the authors included insight from their own clinical experience.
Results CT allows for accurate measurement of the mitral annulus with high special and adequate temporal resolution in all cardiac phases. Therefore, CT represents a valuable method for accurate prosthesis-sizing.
In addition to that, CT can provide information about the valvular- and outflow-tract-anatomy, mitral valve calcifications, configuration of the papillary muscles and of the left ventricle. Additionally, the interventional access-route may concomitantly be visualized.
Conclusion CT plays, in addition to echocardiographic imaging, a central role in pre-interventional assessment prior to TMVR. Especially the precise depiction of the left ventricular outflow tract (LVOT) provides relevant additional information, which is very difficult or not possible to be acquired in their entirety with other imaging modalities.
Key Points:
-
CT plays a central role in pre-interventional imaging for TMVR.
-
CT-measurements allow for accurate prosthesis-sizing.
-
CT provides valuable information about LVOT-anatomy, mitral calcifications and interventional access-route.
Citation Format
-
Heiser L, Gohmann RF, Noack T et al. CT Planning prior to Transcatheter Mitral Valve Replacement (TMVR). Fortschr Röntgenstr 2022; 194: 373 – 383
Key words
TMVI - TMVR - transcatheter mitral valve implantation - transcatheter mitral valve replacement - computed tomography - CTIntroduction
Mitral valve regurgitation (MR) represents the most common valvular cardiac disease in the western world. Prevalence is age-dependent and increases with age; above the age of 75 years, it increases to as much as 10 % in the normal population [1].
The origin can be classified as either primary or secondary MR. Primary MR is due to degenerative or destructive causes resulting in pathological changes in the valve annulus and leaflets and ultimately to inadequate valve closure. The most common cause is mitral valve prolapse [2]. Secondary insufficiency generally occurs in the course of annulus dilation due to left atrial dilation (atrial mitral insufficiency) or alteration of left ventricular geometry as consequence of primary or secondary cardiomyopathy [3] [4].
According to the current European treatment guidelines, early surgical mitral valve repair or surgical valve replacement is primarily recommended in patients with symptomatic high-grade primary MR and left ventricular ejection fraction (LVEF) > 30 %. Optimization of drug therapy is recommended first in patients with severely impaired LVEF (< 30 %). In the absence of successful therapy, surgical or interventional therapy may be performed after interdisciplinary decision making in the Heart Team. Interventional or surgical treatment of secondary MR is the subject of ongoing debate. Thus, in current treatment recommendations, surgical therapy is recommended only when bypass surgery is performed simultaneously and LVEF > 30 % (class I, level of evidence C). Surgical mitral valve therapy alone may be considered if LVEF < 30 % and operative risk is low (class IIa, level of evidence C). If the operative risk is increased, interventional reconstruction/replacement may be considered (class IIb, level of evidence C) [5].
Due to the increasing prevalence of MR in older age and the associated rise in surgical risk, different interventional procedures have been developed as an alternative to drug or surgical therapy alone. Various approaches are available for interventional treatment of the mitral valve. A basic distinction can be made between transcatheter mitral valve repair and transcatheter mitral valve replacement (TMVR). According to their therapeutic approach, reconstructive interventional procedures can be divided into ring annuloplasty (e. g. Cardioband), coaptation (e. g. MitraClip, PASCAL), and neochord (e. g. NeoChord, Harpoon) procedures [6]. All procedures are subject to anatomical and morphological selection criteria. If these are not met, TMVR is another treatment option.
In addition to treating MR, transcatheter mitral valve replacement (TMVR) can also be used to treat calcified mitral valve stenosis or as part of a “valve-in-ring” or “valve-in-valve” procedure [7].
Specific measurements of the complex three-dimensional anatomy of the mitral valve annulus and surrounding structures are necessary for pre-interventional planning of a TMVR; a CT examination with ECG gating is a suitable method for this due to its high spatial and adequate temporal resolution.
CT shows higher reliability compared to echocardiography with respect to the measurement of the annulus and sizing of the prosthetic valve [8]. The key advantage of CT scanning over other non-invasive imaging modalities is the ability to visualize the entire cardiac anatomy, including the coronary arteries and the potential access routes as well as the estimation of the postinterventionally altered left ventricular outflow tract (“neo-LVOT”) in a single examination within a few seconds.
Features of Mitral Valve Anatomy
The mitral valve consists of two connective tissue leaflets, an anterior (AML) and posterior (PML) mitral valve leaflet, each of which can be subdivided into three segments ([Fig. 1]). Both valve leaflets merge at the medial and lateral commissure. In addition to the leaflets, the functional unit of the mitral valve is completed by the annulus as well as the holding mechanism. The anterior third of the annulus is formed by the fibrous component, at the end of which there are two connective tissue-compacted areas: the medial and lateral trigonum. These trigones, together with the AML and through their direct relationship to the aortic valve and the left ventricular outflow tract (LVOT), form what is known as the aortomitral continuity. The posterior two-thirds form the muscular portion of the annulus. The subvalvular portion of the valve is composed of the chordae tendineae and papillary muscles that connect the mitral valve leaflets to the left ventricular myocardium [9] [10] [11].

The complexity of the mitral valve anatomy is based on the saddle-shaped three-dimensional dynamic form of the annulus ([Fig. 2a, b]). This saddle-shaped annulus has its highest point in the middle of the anterior third and extends to the level of the aortic valve, more specifically to the insertion of the left coronary and the acoronary cusp. Another, smaller elevation is found at the insertion of the posterior leaflet. The lowest points of the annulus are formed by the trigones [12] [13].

Available Devices
Challenges to secure placement and anchoring of the prosthesis during TMVR include the complex anatomy of the mitral valve, annulus dynamics and aortomitral continuity. For example, the annulus increases in size by up to 20 % during systole [14]. In addition, implantation of the prosthesis carries the risk of obstruction because of the close spatial relationship of the mitral valve annulus to the LVOT.
The various conceivable solutions for taking these anatomical and physiological conditions into account result in a variety of devices which differ, for example, by the anchoring mechanism and in their position relative to the annulus ([Table 1, ] [Fig. 3]).
Overview of commonly used valve prostheses for TMVR, their complications rates and important parameters regarding implantation/planning (modified from Ranganath et al. [10] (TVMR = transcatheter mitral valve replacement, LVOT = left ventricular outflow tract, AP = Anterior-posterior diameter, LM = Lateromedial diameter, N/A = not available).

At this time, there are more than 30 devices available, some of which are summarized in [Table 1] [10] [15] [16] [17] [18]. Currently the most common one is the Tendyne device (Abbott Cardiovascular, Plymouth, USA), which is the only apparatus with CE certification for use in routine clinical practice. In addition, off-label use with a prosthesis for transcatheter aortic valve implantation, e. g., the Sapien 3 (Edwards Lifesciences, Inc., Irvine, CA, USA), is also possible [19]. Other devices are currently undergoing clinical trials.
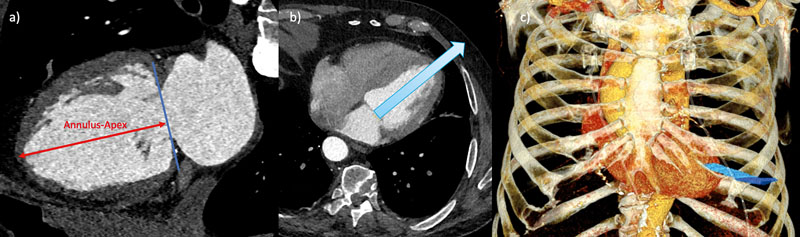
The chosen access route should be as perpendicular as possible to the annulus in order to achieve optimal deployment and anchorage of the device, thus reducing the risk of LVOT obstruction or paravalvular leak. On the one hand, a transapical approach can be selected, since the imaginary central axis between annulus and apex of the left ventricle (LV) can usually be projected well and determined by CT ([Fig. 4]) [20] [21] [22] [23]. On the other hand, the less invasive transfemoral-transseptal access is also an option for prosthesis implantation, which does not require opening of the thorax by mini-thoracotomy as in the transapical approach, thus allowing a purely endovascular procedure [24]. In the context of transseptal puncture, CT can provide helpful additional information for visualizing the best possible procedure regarding access to the left atrium and mitral valve [10].

In a 2017 meta-analysis by del Val et al., the proportion of successful implantations in the reviewed studies was approximately 92 % of the total procedures performed. LVOT obstruction was observed in only 0.4 % of patients [25].
CT Scanning Protocol
A CT scanner with the highest possible temporal resolution is advantageous due to the need to visualize heart structures as artifact-free as possible throughout the cardiac cycle.
With only a few exceptions, a helical scan of the heart with retrospective ECG gating should be employed in order to allow measurement in multiple cardiac phases and to create dynamic reconstructions of mitral valve motion as a moving image series over the cardiac cycle. Supplemental cardiac calcium scoring should be considered to plan the cardiac scan window and positively identify mitral valve calcifications [26].
Additionally, a depiction of the anticipated access route is useful. If a transapical approach is anticipated, supplementary imaging or reconstruction of the thorax may be helpful.
Optimally, imaging of cardiac anatomy should be performed as a helical scan of the heart using retrospective ECG gating immediatly followed by an untriggered scan utilizing the same contrast bolus for imaging of the access pathway. In order to achieve sufficient contrast, it is recommended to adapt the amount of contrast medium to the scan time and, if necessary, the patient’s cardiac output. The typically flattened contrast kinetics in patients with high-grade MR can be counteracted with an appropriately high flow rate (> 5 ml/s).
Cardiac scan reconstruction should be performed in 5 % increments with respect to the RR interval and the use of the smallest possible slice thickness and increment is recommended.
To shorten the switching time, it may be useful to vary the scan direction so that the helical scan of the heart is performed in caudocranial scan direction and remaining volume is scanned in the opposite direction.
Using a scan mode with retrospective ECG gating provides a comparatively high probability for possibly diagnostic assessment of the coronary arteries since correction of arrhythmias can be achieved via manual editing of the ECG-based reconstruction parameters [27]. Furthermore, even with higher heart rates or arrhythmia, diagnostic coronary imaging is more likely to be possible in this scan mode compared to using prospective ECG triggering [28]. Therefore, evaluation of a CT scan for planning TMVR should include assessment of the coronary arteries with respect to anomalies and possible stenosis.
Saddle vs. D-Shape
Accurate measurement of the mitral valve annulus is the focus of preinterventional CT planning. The anatomically saddle-shaped form of the annulus makes it difficult to establish a two-dimensional plane that can be easily measured. Therefore, it is advantageous to simplify the complex 3-dimensional shape of the annulus to a 2-dimensional contour by projecting suitable landmarks. This projection takes the simplified form of a virtual “D” ([Fig. 2c, d]). With this “D-shaped” configuration the trigona fibrosa are connected by a virtual line and the anterior horn, which is not contained in the two-dimensional plane, is neglected [11] [12]. Looking at the shape of the most commonly used devices, such as Tiara or Tendyne, the cross-section at the level of the landing zone also corresponds most closely to a “D-shaped” configuration. Likewise, use of the D-shape is advantageous with respect to the correct evaluation of a possible LVOT obstruction. Neglecting the anterior horn reduces the probability of an oversized prosthesis, while assuming an approximately tubular deployment of the prosthesis allows for a more realistic representation of the actual position of the implanted device, especially with regard to the positional relationship to the LVOT or the assumed configuration of the “neo-LVOT” after implantation [29].
Step-by-Step Instructions
To set the correct annulus plane, it is useful to have dedicated postprocessing software that allows the preparation of multiplanar reconstructions (MPR) in several planes. However, this can also be done with most radiological image storage and communication systems (PACS). For this purpose, it is recommended to link the related planes and visualize their alignment using a crosshair.
[Fig. 5] illustrates an image-by-image representation of the previously described steps.

Step 1 (a–c): Rough approach to the mitral valve plane. The crosshairs are centered on the middle of the mitral valve plane (a). Subsequently, the second and third planes (b, c) are aligned along the AV valve plane. A rough orientation to the LV apex is helpful for alignment in basal-apical direction.
Step 2 (d–f): Setting the left trigonum. In the short-axis view, the location of the left trigonum is identified and put in the crosshairs are (white arrow in d, e, f). When set correctly, it is shown as a triangularly configured, clearly defined structure.
Step 3 (g–i): Setting the right trigonum. By rotating the second plane (i), the right trigonum fibrosum (white arrow in g, h, i) is also adjusted in short axis view (g) until it can be seen as a clearly delineated triangular structure. Once this is achieved, TT and thus the septal contour of the mitral valve annulus are correctly set.
Step 4 (j–l): Setting the lateral annulus contour. In the short axis (j), the crosshairs are set to the TT. The lateral annulus contour (purple arrows in j) is now adjusted in the second plane (k, l) until a D-shape is seen in short axis view (j) and the lateral contour is completely occupied by the mitral valve annulus. (TT = inter-trigonal distance, AV valve plane = atrioventricular valve plane).
This created sectional plane now allows the determination of the relevant measurement values for sizing of the valve prosthesis ([Fig. 6]), which should be performed in an analogous manner in systole and diastole.

The most common measured values to be determined are shown in [Fig. 6] and summarized in List 1 [29].
Risk Factors of LVOT Obstruction
Proper selection of prosthesis type and size is important, since LVOT obstruction is a potential and relevant complication of TMVR.
The native LVOT is located between the basal interventricular septum and the aortomitral continuity ([Fig. 7a]). Due to protrusion of the prosthesis into the left ventricle, the resulting elongation of the native LVOT and interaction with the AML result in the formation of a so-called “neo-LVOT” ([Fig. 7b, c]).

The risk of obstruction grows with increasing size and protrusion of the device. According to the current state of knowledge, limit values for the area of the “neo-LVOT” are 1.7–1.9 cm2 and are device-specific [30].
Patient-specific characteristics included aortomitral angulation ([Fig. 7 d]), left ventricular dimension and basal septal thickness ([Table 1]).
Aortomitral angulation influences the subsequent position and alignment of the prosthesis and describes the angle between the respective orthogonals to the mitral and aortic valve planes ([Fig. 7 d]). Theoretically, an approximately parallel alignment of both axes would be optimal, whereas the risk of obstruction increases significantly if this approaches or exceeds 90° [29] [31].
Hypertrophy of the basal interventricular septum (> 15 mm) may also lead to narrowing of the LVOT (or “neo-LVOT”). In addition, a small left ventricular cavity is another risk factor in this regard. In patients with secondary MR, the LV is usually clearly dilated, whereas in patients with primary MR the mostly hyperdynamic LV function leads to a systolic reduction in the LV cavity [12].
Landing Zone
CT also provides information on the so-called landing zone of the device, which is influenced by numerous factors such as the presence/distribution of annular calcification or the development of a myocardial shelf.
Myocardial shelf
The anatomical difference between the landing zone in primary and secondary MR is important in pre-interventional planning. Secondary MR is often associated with regional wall movement disorders and dilation of the LV, which leads to displacement of the papillary muscles as well as ultimately to annulus dilation. Furthermore, remodeling of the basal myocardium also disrupts the actual linear connection between the left atrial and left ventricular myocardium, resulting in the so-called “myocardial shelf”. The size of the “myocardial shelf” depends on several factors; typically, it is largest in the presence of LV dilation combined with posterior wall infarction. Importantly, the “myocardial shelf” is also subject to dynamic size change and may even disappear altogether during systole. Determining the exact extent of the myocardial shelf is important because some self-expanding systems require a persistent shelf for anchorage. In patients with primary MR, there is typically no “myocardial shelf” present [29] [32] [33].
Mitral valve calcification
Calcification of the mitral valve annulus, trigona fibrosa or valve leaflets may also influence intervention planning and can be well visualized by CT ([Fig. 8]). Generally, calcifications are found in the posterior portion of the annulus fibrosus and are particularly present in elderly patients [34] [35].

Computed tomographic imaging in short-axis view ([Fig. 8a]) is particularly suitable for describing calcifications. According to Guerrero et al. [36] an association was found between minor calcifications of the mitral valve and an increased likelihood of migration of the TMVR device; a score was used for quantification and standardized recording of the calcifications. This score refers to the thickness of annular calcifications, their extension in relation to the circumference, the involvement of the trigona and the valve leaflets [36].
Annulus-Apex Connection
The orientation and length of the annulus-apex line represent ([Fig. 4a]) additional relevant information for TMVR planning. To achieve this, an orthogonal connecting line is drawn from the center of the mitral valve plane to the epicardial contour of the LV apex ([Fig. 4a]) [31]. This facilitates the planning of a transapical access route, since the necessary length and orientation of the delivery system can be assessed here ([Fig. 4]).
The location of the LV apex with respect to the center of the mitral valve plane may vary from patient to patient [31]. Visualization of the actual anatomy can provide information on whether deviating from a strictly transapical access path will allow better alignment of the delivery system.
In extension of the annulus apex line, the corresponding intercostal space should be indicated where it intersects the thoracic wall ([Fig. 4b]). This may be helpful in planning the exact transapical access route. A 3 D reconstruction is particularly suitable for illustration ([Fig. 4c]).
Report and Documentation
Due to the complexity of the evaluation, the use of a standardized report template and uniform image documentation is recommended to increase clarity and comprehensiveness of the report.
On the one hand, MPRs in short-axis view and in 2- and 3-chamber view should be prepared for general overview. On the other hand, moving image series over the cardiac cycle along the mitral valve annulus and in 2-chamber and 3-chamber view should also be obtained to visualize the dynamic and anatomical changes within the cardiac cycle.
It is recommended that measurement of the mitral valve annulus should be performed using the standardized mitral valve plane setting in “D-Shape”, as described previously.. An overview of relevant measured values can be found in List 1; these should also be documented as image findings.
Mitral annulus (diastolic and systolic measurements)
-
TT, AP, LM
-
perimeter and area
-
leaflet morphology
Additional parameters
LVOT (diastolic and systolic measurements)
-
minimal/maximal diameter
-
perimeter and Area
-
aortomitral angulation
-
enddiastolic septum thickness
-
minimal LV-diameter
Landing zone
-
presence, distribution and quantity of mitral annulus calcifications
-
“myocardial shelf”
Access route
-
transapical: annulus-apex distance, ICS for optimal trajectory
-
transfemoral-transseptal: course of Vv. femorales, Vv. Iliacales and V. cava inferior
Other aspects
Coronary arteries
-
In case of diagnostic depicted coronary arteries: Rule-out of obstructive CAD possible?
-
(If desired Calcium-Score)
Thorax/abdomen
-
Other pathological findings in the scanned volume?
(TMVR = transcatheter mitral valve replacement, TT = inter-trigonal distance, AP = anterior-posterior diameter, LM = lateral-medial diameter, ICS = intercostal space, LV = left ventricle, LVOT = left ventricular outflow tract, CAD = coronary artery disease).
Summary
CT represents the central imaging modality for TMVR planning. With this imaging modality, both a visualization of the anatomical conditions and an individual and patient-centered interventional planning and prosthesis selection are reliably possible.
The mitral valve annulus should be set in a D-shape configuration and using definite anatomical landmarks for reproducibility of two-dimensional sizing. Calcifications of the annulus can be estimated very well using computed tomography and can be easily described with regard to location and distribution.
Furthermore, CT allows detailed visualization of the size and configuration of the LVOT and thus allows estimation of the likelihood of postinterventional LVOT obstruction.
Appropriate visualization capabilities are available for both a transapical and a transfemoral-transseptal approach, allowing planning of the optimal interventional procedure.
The collected measured values and qualitative statements on intervention planning should be recorded in a standardized report.
CT Planning prior to Transcatheter Mitral Valve Replacement (TMVR)
Heiser L, Gohmann RF, Noack T et al. CT Planning prior to Transcatheter Mitral Valve Replacement (TMVR).
Fortschr Röntgenstr 2022; 194: 373–383
Correction on page 374, 375. The correct sentence is: This saddle-shaped annulus has its highest point in the middle of the anterior third and extends to the level of the aortic valve, more specifically to the insertion of the left coronary and the acoronary cusp.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Nkomo VT. et al. Burden of valvular heart diseases: a population-based study. Lancet 2006; 368: 1005-1011
- 2 Nishimura RA, Bonow RO. Percutaneous Repair of Secondary Mitral Regurgitation – A Tale of Two Trials. N Engl J Med 2018; 379: 2374-2376
- 3 Levine RA. et al. Mitral valve disease – morphology and mechanisms. Nat Rev Cardiol 2015; 12: 689-710
- 4 Delgado V. et al. Assessment of mitral valve anatomy and geometry with multislice computed tomography. JACC Cardiovasc Imaging 2009; 2: 556-565
- 5 Baumgartner H. et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev Esp Cardiol (Engl Ed) 2018; 71: 110
- 6 Noack T. et al. Transcatheter mitral valve repair: review of current techniques. Indian J Thorac Cardiovasc Surg 2020; 36 (Suppl. 01) 53-63
- 7 Yoon SH. et al. Transcatheter Mitral Valve Replacement for Degenerated Bioprosthetic Valves and Failed Annuloplasty Rings. J Am Coll Cardiol 2017; 70: 1121-1131
- 8 Binder RK, Webb JG. Percutaneous mitral and aortic paravalvular leak repair: indications, current application, and future directions. Curr Cardiol Rep 2013; 15: 342
- 9 Garbi M, Monaghan MJ. Quantitative mitral valve anatomy and pathology. Echo Res Pract 2015; 2: R63-R72
- 10 Ranganath P. et al. CT for Pre- and Postprocedural Evaluation of Transcatheter Mitral Valve Replacement. Radiographics 2020; 40: 1528-1553
- 11 Blanke P. et al. A simplified D-shaped model of the mitral annulus to facilitate CT-based sizing before transcatheter mitral valve implantation. J Cardiovasc Comput Tomogr 2014; 8: 459-467
- 12 Blanke P. et al. Multimodality Imaging in the Context of Transcatheter Mitral Valve Replacement: Establishing Consensus Among Modalities and Disciplines. JACC Cardiovasc Imaging 2015; 8: 1191-1208
- 13 Asgar AW. Sizing the Mitral Annulus: Is CT the Future?. JACC Cardiovasc Imaging 2016; 9: 281-282
- 14 Noack T. et al. Dynamic mitral valve geometry in patients with primary and secondary mitral regurgitation: implications for mitral valve repairdagger. Eur J Cardiothorac Surg 2019; 56: 983-992
- 15 Muller DWM. et al. Transcatheter Mitral Valve Replacement for Patients With Symptomatic Mitral Regurgitation: A Global Feasibility Trial. J Am Coll Cardiol 2017; 69: 381-391
- 16 Bapat V. et al. Early Experience With New Transcatheter Mitral Valve Replacement. J Am Coll Cardiol 2018; 71: 12-21
- 17 Guerrero M. et al. 1-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol 2018; 71: 1841-1853
- 18 Cheung A. Early experience of TIARA transcatheter mitral valve replacement system. Ann Cardiothorac Surg 2018; 7: 787-791
- 19 Guerrero M. et al. Thirty-Day Outcomes of Transcatheter Mitral Valve Replacement for Degenerated Mitral Bioprostheses (Valve-in-Valve), Failed Surgical Rings (Valve-in-Ring), and Native Valve With Severe Mitral Annular Calcification (Valve-in-Mitral Annular Calcification) in the United States: Data From the Society of Thoracic Surgeons/American College of Cardiology/Transcatheter Valve Therapy Registry. Circ Cardiovasc Interv 2020; 13: e008425
- 20 Vahanian A, Urena M, Himbert D. Transcatheter Mitral Valve Replacement: The End of the Beginning?. J Am Coll Cardiol 2019; 73: 1261-1263
- 21 Sondergaard L. et al Transcatheter mitral valve implantation via transapical approach: an early experience. Eur J Cardiothorac Surg 2015; 48: 873-877 ; discussion 877–878
- 22 Cheung A. et al. Short-term results of transapical transcatheter mitral valve implantation for mitral regurgitation. J Am Coll Cardiol 2014; 64: 1814-1819
- 23 Regueiro A. et al. Transcatheter Mitral Valve Replacement: Insights From Early Clinical Experience and Future Challenges. J Am Coll Cardiol 2017; 69: 2175-2192
- 24 Urena M. et al. Transseptal Transcatheter Mitral Valve Replacement Using Balloon-Expandable Transcatheter Heart Valves: A Step-by-Step Approach. JACC Cardiovasc Interv 2017; 10: 1905-1919
- 25 Del Val D. et al. Early Experience With Transcatheter Mitral Valve Replacement: A Systematic Review. J Am Heart Assoc 2019; 8: e013332
- 26 Leschka S. et al. Scan length adjustment of CT coronary angiography using the calcium scoring scan: effect on radiation dose. Am J Roentgenol 2010; 194: W272-W277
- 27 Gohmann RF. et al. Combined Coronary CT-Angiography and TAVI-Planning: A Contrast-Neutral Routine Approach for Ruling-out Significant Coronary Artery Disease. J Clin Med 2020; 9: 1623
- 28 Seitz P, Gottschling S, Lücke C. et al. Pre-procedural high-pitch coronary CT angiography assessment of patients undergoing transcatheter aortic valve implantation (TAVI) without patient-specific adjustment: analysis of diagnostic performance. Clinical Radiology 2021; 76: 862.e29-862.e36
- 29 Blanke P. et al. Mitral Annular Evaluation With CT in the Context of Transcatheter Mitral Valve Replacement. JACC Cardiovasc Imaging 2015; 8: 612-615
- 30 Reid A. et al. Neo-LVOT and Transcatheter Mitral Valve Replacement: Expert Recommendations. JACC Cardiovasc Imaging 2021; 14: 854-866
- 31 Blanke P. et al. Predicting LVOT Obstruction in Transcatheter Mitral Valve Implantation: Concept of the Neo-LVOT. JACC Cardiovasc Imaging 2017; 10: 482-485
- 32 Naoum C. et al. Mitral Annular Dimensions and Geometry in Patients With Functional Mitral Regurgitation and Mitral Valve Prolapse: Implications for Transcatheter Mitral Valve Implantation. JACC Cardiovasc Imaging 2016; 9: 269-280
- 33 Faggioni L. et al. Preprocedural planning of transcatheter mitral valve interventions by multidetector CT: What the radiologist needs to know. Eur J Radiol Open 2018; 5: 131-140
- 34 Korn D, Desanctis RW, Sell S. Massive calcification of the mitral annulus. A clinicopathological study of fourteen cases. N Engl J Med 1962; 267: 900-909
- 35 Abramowitz Y. et al. Concomitant mitral annular calcification and severe aortic stenosis: prevalence, characteristics and outcome following transcatheter aortic valve replacement. Eur Heart J 2017; 38: 1194-1203
- 36 Guerrero M. et al. A Cardiac Computed Tomography-Based Score to Categorize Mitral Annular Calcification Severity and Predict Valve Embolization. JACC Cardiovasc Imaging 2020; 13: 1945-1957
- 37 Capoulade R. et al. Multimodality imaging assessment of mitral valve anatomy in planning for mitral valve repair in secondary mitral regurgitation. J Thorac Dis 2017; 9 (Suppl. 07) S640-S660
Correspondence
Publication History
Received: 30 July 2021
Accepted: 09 November 2021
Article published online:
10 March 2022
© 2022. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Nkomo VT. et al. Burden of valvular heart diseases: a population-based study. Lancet 2006; 368: 1005-1011
- 2 Nishimura RA, Bonow RO. Percutaneous Repair of Secondary Mitral Regurgitation – A Tale of Two Trials. N Engl J Med 2018; 379: 2374-2376
- 3 Levine RA. et al. Mitral valve disease – morphology and mechanisms. Nat Rev Cardiol 2015; 12: 689-710
- 4 Delgado V. et al. Assessment of mitral valve anatomy and geometry with multislice computed tomography. JACC Cardiovasc Imaging 2009; 2: 556-565
- 5 Baumgartner H. et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev Esp Cardiol (Engl Ed) 2018; 71: 110
- 6 Noack T. et al. Transcatheter mitral valve repair: review of current techniques. Indian J Thorac Cardiovasc Surg 2020; 36 (Suppl. 01) 53-63
- 7 Yoon SH. et al. Transcatheter Mitral Valve Replacement for Degenerated Bioprosthetic Valves and Failed Annuloplasty Rings. J Am Coll Cardiol 2017; 70: 1121-1131
- 8 Binder RK, Webb JG. Percutaneous mitral and aortic paravalvular leak repair: indications, current application, and future directions. Curr Cardiol Rep 2013; 15: 342
- 9 Garbi M, Monaghan MJ. Quantitative mitral valve anatomy and pathology. Echo Res Pract 2015; 2: R63-R72
- 10 Ranganath P. et al. CT for Pre- and Postprocedural Evaluation of Transcatheter Mitral Valve Replacement. Radiographics 2020; 40: 1528-1553
- 11 Blanke P. et al. A simplified D-shaped model of the mitral annulus to facilitate CT-based sizing before transcatheter mitral valve implantation. J Cardiovasc Comput Tomogr 2014; 8: 459-467
- 12 Blanke P. et al. Multimodality Imaging in the Context of Transcatheter Mitral Valve Replacement: Establishing Consensus Among Modalities and Disciplines. JACC Cardiovasc Imaging 2015; 8: 1191-1208
- 13 Asgar AW. Sizing the Mitral Annulus: Is CT the Future?. JACC Cardiovasc Imaging 2016; 9: 281-282
- 14 Noack T. et al. Dynamic mitral valve geometry in patients with primary and secondary mitral regurgitation: implications for mitral valve repairdagger. Eur J Cardiothorac Surg 2019; 56: 983-992
- 15 Muller DWM. et al. Transcatheter Mitral Valve Replacement for Patients With Symptomatic Mitral Regurgitation: A Global Feasibility Trial. J Am Coll Cardiol 2017; 69: 381-391
- 16 Bapat V. et al. Early Experience With New Transcatheter Mitral Valve Replacement. J Am Coll Cardiol 2018; 71: 12-21
- 17 Guerrero M. et al. 1-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol 2018; 71: 1841-1853
- 18 Cheung A. Early experience of TIARA transcatheter mitral valve replacement system. Ann Cardiothorac Surg 2018; 7: 787-791
- 19 Guerrero M. et al. Thirty-Day Outcomes of Transcatheter Mitral Valve Replacement for Degenerated Mitral Bioprostheses (Valve-in-Valve), Failed Surgical Rings (Valve-in-Ring), and Native Valve With Severe Mitral Annular Calcification (Valve-in-Mitral Annular Calcification) in the United States: Data From the Society of Thoracic Surgeons/American College of Cardiology/Transcatheter Valve Therapy Registry. Circ Cardiovasc Interv 2020; 13: e008425
- 20 Vahanian A, Urena M, Himbert D. Transcatheter Mitral Valve Replacement: The End of the Beginning?. J Am Coll Cardiol 2019; 73: 1261-1263
- 21 Sondergaard L. et al Transcatheter mitral valve implantation via transapical approach: an early experience. Eur J Cardiothorac Surg 2015; 48: 873-877 ; discussion 877–878
- 22 Cheung A. et al. Short-term results of transapical transcatheter mitral valve implantation for mitral regurgitation. J Am Coll Cardiol 2014; 64: 1814-1819
- 23 Regueiro A. et al. Transcatheter Mitral Valve Replacement: Insights From Early Clinical Experience and Future Challenges. J Am Coll Cardiol 2017; 69: 2175-2192
- 24 Urena M. et al. Transseptal Transcatheter Mitral Valve Replacement Using Balloon-Expandable Transcatheter Heart Valves: A Step-by-Step Approach. JACC Cardiovasc Interv 2017; 10: 1905-1919
- 25 Del Val D. et al. Early Experience With Transcatheter Mitral Valve Replacement: A Systematic Review. J Am Heart Assoc 2019; 8: e013332
- 26 Leschka S. et al. Scan length adjustment of CT coronary angiography using the calcium scoring scan: effect on radiation dose. Am J Roentgenol 2010; 194: W272-W277
- 27 Gohmann RF. et al. Combined Coronary CT-Angiography and TAVI-Planning: A Contrast-Neutral Routine Approach for Ruling-out Significant Coronary Artery Disease. J Clin Med 2020; 9: 1623
- 28 Seitz P, Gottschling S, Lücke C. et al. Pre-procedural high-pitch coronary CT angiography assessment of patients undergoing transcatheter aortic valve implantation (TAVI) without patient-specific adjustment: analysis of diagnostic performance. Clinical Radiology 2021; 76: 862.e29-862.e36
- 29 Blanke P. et al. Mitral Annular Evaluation With CT in the Context of Transcatheter Mitral Valve Replacement. JACC Cardiovasc Imaging 2015; 8: 612-615
- 30 Reid A. et al. Neo-LVOT and Transcatheter Mitral Valve Replacement: Expert Recommendations. JACC Cardiovasc Imaging 2021; 14: 854-866
- 31 Blanke P. et al. Predicting LVOT Obstruction in Transcatheter Mitral Valve Implantation: Concept of the Neo-LVOT. JACC Cardiovasc Imaging 2017; 10: 482-485
- 32 Naoum C. et al. Mitral Annular Dimensions and Geometry in Patients With Functional Mitral Regurgitation and Mitral Valve Prolapse: Implications for Transcatheter Mitral Valve Implantation. JACC Cardiovasc Imaging 2016; 9: 269-280
- 33 Faggioni L. et al. Preprocedural planning of transcatheter mitral valve interventions by multidetector CT: What the radiologist needs to know. Eur J Radiol Open 2018; 5: 131-140
- 34 Korn D, Desanctis RW, Sell S. Massive calcification of the mitral annulus. A clinicopathological study of fourteen cases. N Engl J Med 1962; 267: 900-909
- 35 Abramowitz Y. et al. Concomitant mitral annular calcification and severe aortic stenosis: prevalence, characteristics and outcome following transcatheter aortic valve replacement. Eur Heart J 2017; 38: 1194-1203
- 36 Guerrero M. et al. A Cardiac Computed Tomography-Based Score to Categorize Mitral Annular Calcification Severity and Predict Valve Embolization. JACC Cardiovasc Imaging 2020; 13: 1945-1957
- 37 Capoulade R. et al. Multimodality imaging assessment of mitral valve anatomy in planning for mitral valve repair in secondary mitral regurgitation. J Thorac Dis 2017; 9 (Suppl. 07) S640-S660
Step 1 (a–c): Rough approach to the mitral valve plane. The crosshairs are centered on the middle of the mitral valve plane (a). Subsequently, the second and third planes (b, c) are aligned along the AV valve plane. A rough orientation to the LV apex is helpful for alignment in basal-apical direction.
Step 2 (d–f): Setting the left trigonum. In the short-axis view, the location of the left trigonum is identified and put in the crosshairs are (white arrow in d, e, f). When set correctly, it is shown as a triangularly configured, clearly defined structure.
Step 3 (g–i): Setting the right trigonum. By rotating the second plane (i), the right trigonum fibrosum (white arrow in g, h, i) is also adjusted in short axis view (g) until it can be seen as a clearly delineated triangular structure. Once this is achieved, TT and thus the septal contour of the mitral valve annulus are correctly set.
Step 4 (j–l): Setting the lateral annulus contour. In the short axis (j), the crosshairs are set to the TT. The lateral annulus contour (purple arrows in j) is now adjusted in the second plane (k, l) until a D-shape is seen in short axis view (j) and the lateral contour is completely occupied by the mitral valve annulus. (TT = inter-trigonal distance, AV valve plane = atrioventricular valve plane).




Schritt 1 (a–c): Grobe Annäherung an die Mitralklappen-Ebene: Das Fadenkreuz wird auf die Mitte der Mitralklappenebene zentriert (a). Anschließen werden die zweite und dritte (b, c) Ebene entlang der AV-Klappenebene ausgerichtet. Hilfreich für die Ausrichtung in basal-apikaler Richtung ist eine grobe Orientierung zum LV-Apex.
Schritt 2 (d–f): Einstellung des linken Trigonums: Im Kurzachsenschnitten wird die Lokalisation des linken Trigonums identifiziert und das Fadenkreuz hierauf eingestellt (weißer Pfeil in d, e, f). Dieses stellt sich bei korrekter Einstellung als triangulär konfigurierte, klar definierte Struktur dar.
Schritt 3 (g–i): Einstellung des rechten Trigonums: Durch Rotieren der zweiten Ebene (i) wird in der Kurzachse (g) auch das rechte Trigonum fibrosum (weißer Pfeil in g, h, i) so eingestellt, bis es als klar abgrenzbare, trianguläre Struktur zu erkennen ist. Sobald dies erfolgt ist, sind TT und somit die Septum-seitige Kontur des Mitralklappen-Annulus korrekt eingestellt.
Schritt 4 (j–l): Einstellung der lateralen Annuluskontur: In der Kurzachse (j) wird das Fadenkreuz auf die TT eingestellt.


