

Subscribe to RSS
DOI: 10.1055/a-1071-7527
Esophageal muscle layer tear during endoscopic submucosal dissection treated by polyglycolic acid sheets and fibrin glue
Authors

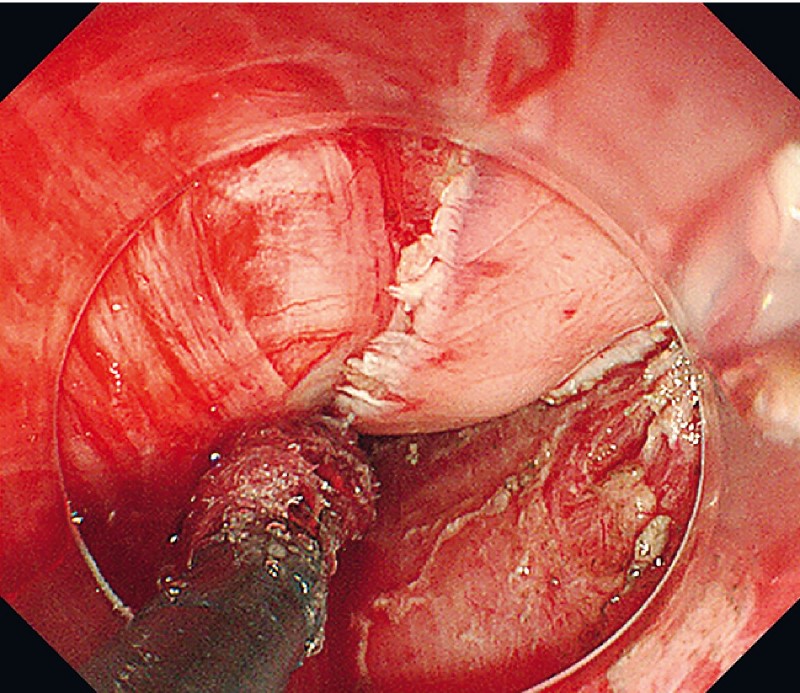
An 88-year-old woman was referred to our hospital because of esophageal squamous cell carcinoma that had been detected by esophagogastroduodenoscopy. Computed tomography (CT) showed no abnormalities. Endoscopy revealed a half-circumferential, subtle, reddish lesion on the left side of the middle esophagus ([Video 1]). Chromoendoscopy with iodine dye made the lesion clear as an unstained area ([Fig. 1]). Endoscopic submucosal dissection (ESD) with carbon dioxide insufflation was performed. During the ESD procedure, massive gas insufflations were repeated many times because of poor endoscopic view. When en bloc resection was completed, endoscopy revealed a proper muscle layer tear on the anterior side of the ESD ulcer, and the epicardium was seen through the muscle layer tear ([Fig. 2], arrows). Massive gas insufflation may cause blunt injury to muscle tissue. By using a grasping forceps, a total of ten 1 cm × 1 cm polyglycolic acid (PGA) sheets were delivered to the site and attached by fibrin glue ([Fig. 3] and [Fig. 4]). In addition, CT showed free air and fluid collection in the mediastinum. Therefore, we administered antibiotics as well as continuous esophageal suction by a nasogastric tube for 1 week. The lesion had been resected completely, and histological examination revealed squamous cell carcinoma confined to the lamina propria mucosae. Periodic endoscopic examinations showed the healing course of the post-ESD ulcer. The ulcer healed completely without signs of cancer recurrence at 10 weeks post-ESD ([Fig. 5]).
Video 1 Esophageal muscle layer tear during endoscopic submucosal dissection (ESD) treated with polyglycolic acid (PGA) sheets and fibrin glue endoscopically.




Perforation is one of the major complications of ESD [1]. A proper muscle layer tear might be considered the same as a perforation in Boerhaave syndrome, which results in a sudden increase in intraesophageal pressure [2]. PGA sheets are used in endoscopic techniques for the closure of gastrointestinal perforations [3] [4] [5]. In the current case, the mucosal and muscular defect after esophageal ESD was treated with PGA sheets and fibrin glue.
Endoscopy_UCTN_Code_CPL_1AH_2AZ
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
* Contributed equally as first authors
-
References
- 1 Yamamoto Y, Kikuchi D, Nagami Y. et al. Management of adverse events related to endoscopic resection of upper gastrointestinal neoplasms: Review of the literature and recommendations from experts. Dig Endosc 2019; 31 (Suppl. 01) 4-20
- 2 Pate JW, Walker WA, Cole Jr. FH. et al. Spontaneous rupture of the esophagus: a 30-year experience. Ann Thorac Surg 1989; 47: 689-692
- 3 Takimoto K, Imai Y, Matsuyama K. Endoscopic tissue shielding method with polyglycolic acid sheets and fibrin glue to prevent delayed perforation after duodenal endoscopic submucosal dissection. Dig Endosc 2014; 26 (Suppl. 02) 46-49
- 4 Sakaguchi Y, Tsuji Y, Yamamichi N. et al. Successful closure of a large perforation during colorectal endoscopic submucosal dissection by application of polyglycolic acid sheets and fibrin glue. Gastrointest Endosc 2016; 84: 374-375
- 5 Seehawong U, Morita Y, Nakano Y. et al. Successful treatment of an esophageal perforation that occurred during endoscopic submucosal dissection for esophageal cancer using polyglycolic acid sheets and fibrin glue. Clin J Gastroenterol 2019; 12: 29-33
Corresponding author
-
References
- 1 Yamamoto Y, Kikuchi D, Nagami Y. et al. Management of adverse events related to endoscopic resection of upper gastrointestinal neoplasms: Review of the literature and recommendations from experts. Dig Endosc 2019; 31 (Suppl. 01) 4-20
- 2 Pate JW, Walker WA, Cole Jr. FH. et al. Spontaneous rupture of the esophagus: a 30-year experience. Ann Thorac Surg 1989; 47: 689-692
- 3 Takimoto K, Imai Y, Matsuyama K. Endoscopic tissue shielding method with polyglycolic acid sheets and fibrin glue to prevent delayed perforation after duodenal endoscopic submucosal dissection. Dig Endosc 2014; 26 (Suppl. 02) 46-49
- 4 Sakaguchi Y, Tsuji Y, Yamamichi N. et al. Successful closure of a large perforation during colorectal endoscopic submucosal dissection by application of polyglycolic acid sheets and fibrin glue. Gastrointest Endosc 2016; 84: 374-375
- 5 Seehawong U, Morita Y, Nakano Y. et al. Successful treatment of an esophageal perforation that occurred during endoscopic submucosal dissection for esophageal cancer using polyglycolic acid sheets and fibrin glue. Clin J Gastroenterol 2019; 12: 29-33