

Subscribe to RSS
DOI: 10.1055/a-0919-4249
Endoscopic resection of a large adenocarcinoma involving the appendix using a full-thickness resection device
Authors
Corresponding author
Publication History
Publication Date:
01 July 2019 (online)

The endoscopic treatment of adenomas involving the appendiceal orifice with endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) is a big challenge, even for experienced endoscopists, because of the high risks of incomplete resection and perforation [1] [2] [3]. To date, these lesions have usually required surgical therapy, for example ileocecal resection. Endoscopic full-thickness resection (EFTR) using a full-thickness resection device (FTRD; Ovesco, Tübingen, Germany) was introduced in 2011. Since 2014, the device has had a Conformité Européene (CE) mark and been commercially available in Europe. The device has been well investigated in several studies [4] [5] and one indication for its use is lesions involving the appendix [4] [5].
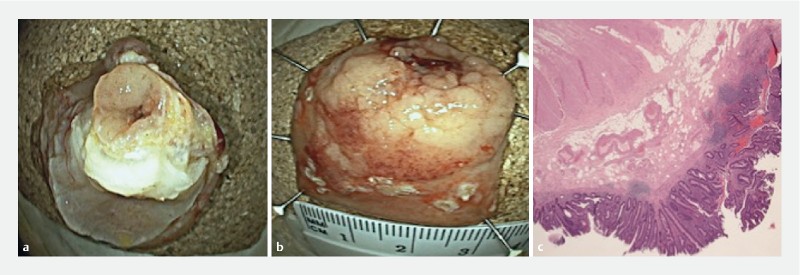
We present the case of a large laterally spreading tumor (LST) invading the appendectomy site ([Fig. 1]). A staging computed tomography (CT) scan of the chest, abdomen, and pelvis did not reveal any distant metastases or other masses. The resection procedure was performed with the patient under deep sedation (continuous propofol infusion) without endotracheal intubation. The patient received prophylactic antibiotic therapy with intravenous ciprofloxacin and metronidazole.

The lateral margins of the lesion were marked with argon plasma coagulation (25 W; Erbe APC 300) ([Fig. 2 a]). To facilitate the introduction of the FTRD, a stiff guidewire was left in the cecum (Jagwire Guidewire ST Stiff; Boston Scientific) ([Fig. 2 b]). The over-the-scope clip (OTSC) device was mounted on the tip of the colonoscope (EC 760 R; Fujifilm). The target lesion was grasped and pulled into the cap using grasping forceps ([Fig. 2 c]) and EFTR was performed ([Fig. 2 d]; [Video 1]).

Video 1 A full-thickness resection of a large laterally spreading tumor involving the appendix is performed using a full-thickness resection device.
After the procedure, the patient developed acute appendicitis 12 hours later, which was treated conservatively with medical therapy. Histology subsequently revealed a carcinoma in situ ([Fig. 3]).
The risk of acute appendicitis after the closure of the appendiceal orifice with the FTRD is real and conservative treatment is certainly the best therapeutic choice. We are firmly convinced of the importance of the discussion with the patient prior to this procedure and of multidisciplinary management.
Endoscopy_UCTN_Code_TTT_1AQ_2AD
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
None
-
References
- 1 Jacob H, Toyonaga T, Ohara Y. et al. Endoscopic submucosal dissection of cecal lesions in proximity to the appendiceal orifice. Endoscopy 2016; 48: 829-836
- 2 Tate DJ, Desomer L, Awadie H. et al. EMR of laterally spreading lesions around or involving the appendiceal orifice: technique, risk factors for failure, and outcomes of a tertiary referral cohort (with video). Gastrointest Endosc 2018; 87: 1279-1288.e2
- 3 Song EM, Yang HJ, Lee HJ. et al. Endoscopic resection of cecal polyps involving the appendiceal orifice: A KASID multicenter study. Dig Dis Sci 2017; 62: 3138-3148
- 4 Schmidt A, Beyna T, Schumacher B. et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018; 67: 1280-1289
- 5 Bronzwaer MES, Bastiaansen BAJ, Koens L. et al. Endoscopic full-thickness resection of polyps involving the appendiceal orifice: a prospective observational case study. Endosc Int Open 2018; 6: E1112-E1119
Corresponding author
-
References
- 1 Jacob H, Toyonaga T, Ohara Y. et al. Endoscopic submucosal dissection of cecal lesions in proximity to the appendiceal orifice. Endoscopy 2016; 48: 829-836
- 2 Tate DJ, Desomer L, Awadie H. et al. EMR of laterally spreading lesions around or involving the appendiceal orifice: technique, risk factors for failure, and outcomes of a tertiary referral cohort (with video). Gastrointest Endosc 2018; 87: 1279-1288.e2
- 3 Song EM, Yang HJ, Lee HJ. et al. Endoscopic resection of cecal polyps involving the appendiceal orifice: A KASID multicenter study. Dig Dis Sci 2017; 62: 3138-3148
- 4 Schmidt A, Beyna T, Schumacher B. et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018; 67: 1280-1289
- 5 Bronzwaer MES, Bastiaansen BAJ, Koens L. et al. Endoscopic full-thickness resection of polyps involving the appendiceal orifice: a prospective observational case study. Endosc Int Open 2018; 6: E1112-E1119