

Subscribe to RSS
DOI: 10.1055/a-0643-4524
Ultrasound Evaluation of Testicular Volume in Patients with Testicular Microlithiasis
Authors


Abstract
Purpose Ultrasonography is a useful tool to measure testicular volume. According to the European Society of Urogenital Radiology, the combination of testicular atrophy and testicular microlithiasis (TML) is a risk factor for testicular cancer. Testicular atrophy is defined as a volume of less than 12 ml. The aim of this study was to compare testicular volume in patients with TML to patients with normal testicular tissue.
Materials and Methods From 2013 to 2015 we included a total of 91 adult patients with TML, and 91 adult patients with normal testicular tissue as a control group. All patients underwent scrotal B-mode ultrasound investigation including measurement of width, length and height in both testicles. Testicular volume was calculated using the formula π/6×length×height×width.
Results The median age for patients with TML was 48 years (range: 19-94 years), and 48 years (range: 20–75 years) in patients with normal tissue. No statistically significant difference was found between total testicular volume (both testes) >30 ml in patients with TML compared to patients without (OR 0.77 (95% CI 0.43-1.38, p=0.37). However, patients with TML tended to have lower testicular volume compared to patients without TML, when investigating testicular volume below 12 ml.
Conclusion Overall, no association was found between testicular volume and TML, but there was a trend indicating that severe atrophy is often seen in patients with TML compared to patients without TML. However, a significant difference was only found in testicular volume ≤8 ml.
Introduction
Testicular microlithiasis (TML) is characterized by the presence of small ultrasonic foci often scattered throughout the testicular parenchyma. Doherty et al. described TML ultrasonographically as innumerable tiny bright echoes diffusely and uniformly scattered throughout their substance [1]. TML is of unknown origin, and typically has a size from 1–3 mm. TML is a painless and impalpable condition only visualized by ultrasonography. The testicles are located extra-abdominal, ideal for superficial high-frequency ultrasound examinations.
Guidelines from the European Society of Urogenital Radiology (ESUR) advocate that TML (five or more microliths per field of view) is considered a risk factor for testicular malignancy when an additional risk factor is present, and annual ultrasound follow-up surveillance is recommended until the age of 55 years [2]. Risk factors are history of maldescent, history of orchidopexy, genetic disease, previous history of germ cell tumor, family history of germ cell tumor, or atrophic testis.
Testicular volume has been investigated in different conditions, e. g. in boys, childhood cryptorchidism, varicocele, testicular germ cell cancer, testicular function, infertility, and Down Syndrome [3] [4] [5] [6] [7] [8] [9]. Ultrasound provides a good and reliable tool for evaluation of testicular volume. It is a method that provides objective, reproducible and accurate measurements, and ultrasonography of the scrotum is a patient-friendly investigation.
Since testicular atrophy is associated with testicular cancer, the objective was to investigate whether atrophy is associated to TML, and the aim of this study was to compare testicular volume in patients with TML and patients with normal testicular tissue.
Materials and Methods
Study population
Patients were included from the Department of Radiology from 2013 to 2015, and all were outpatients referred for an ultrasound of the scrotum by their general practitioner due to symptoms (e. g. testicular pain, swelling, soreness, or nodules). The patients (>18 years) signed an informed consent before entering the study. A total of 101 patients diagnosed with TML were eligible. However, 10 patients had missing measurements from one or both testicles and were excluded. A total of 91 patients with TML were included, and a total of 91 patients with normal testicular tissue served as a control group.
Ultrasound and testicular volume
All ultrasound procedures were carried out with the patient in the supine position. The testicles were investigated in orthogonal transverse and longitudinal planes. All patients underwent b-mode ultrasonography including measurements of maximum height, width and length of both testicles in order to calculate testicular volume ([Fig. 3] and [4]). All ultrasound images were stored in the department’s database Picture Achieve Communication System (PACS, Easyviz Impax Workstation, Medical Insight, Valby, Denmark).
We used a Siemens S3000 ultrasound machine (Acuson Corporation, Siemens, Mountain view, CA, USA), and all scrotal examinations were performed using a linear-array 9L4 frequency transducer with testicular software settings with 50 frames per second, Mechanical Index 1.2, Dynamic range 70, Advanced SieClearTM spatial compounding 5, Dynamic tissue contrast enhancement technology, and tissue harmonic imaging. Four senior radiologists with more than five years of scrotal ultrasound experience performed all of the ultrasound examinations, and all used a standardized procedure. Testicular volume was calculated as π / 6×length (L)×height (H)×width (W). This formula is often used [10] [11] [12].


Ethical approval
The National Data Protection Agency and The Regional Scientific Ethical Committees for Southern Denmark (ID: S-20120144) approved the study.
Statistical methods
All analyses were performed with STATA statistical software (version 15.0 STATA Corporation, College Station, TX, USA).
Results
[Table 1] shows the characteristics in patients with and without TML. The patients were comparable in age. The median age for patients with TML was 48 years (range: 19–94 years), and 48 years (range: 20–75 years) in patients with normal tissue. A total of 11 patients with unilateral TML had additional findings in the unaffected ipsilateral testicle (six testicles with spermatocele, four with hydrocele, and one with varicocele). A total of 33 (36.3%) patients had TML unilateral, and 58 (63.7%) had TML bilateral.
|
TML |
No TML |
Univariate |
|||||||
|---|---|---|---|---|---|---|---|---|---|
|
N |
% |
N |
% |
Odds ratio |
95% CI |
P-value |
|||
|
All Patients |
91 |
100.0 |
91 |
100.0 |
|||||
|
Age |
|||||||||
|
Median age |
48 |
48 |
|||||||
|
≤50 |
53 |
58.2 |
51 |
56.0 |
1.20 |
0.77 |
– |
1.86 |
0.80 |
|
>50 |
38 |
41.8 |
40 |
44.0 |
1.00 |
||||
|
Testicular ultrasound findings |
|||||||||
|
Spermatocele |
13 |
14.3 |
17 |
18.7 |
1.00 |
0.46 |
2.14 |
0.99 |
|
|
Hydrocele |
18 |
19.8 |
17 |
18.7 |
1.38 |
0.68 |
– |
2.80 |
0.38 |
|
Varicocele |
9 |
9.9 |
9 |
9.9 |
1.59 |
0.64 |
– |
3.98 |
0.32 |
|
Testicular cysts |
1 |
1.1 |
1 |
1.1 |
1.30 |
0.08 |
– |
21.1 |
0.85 |
|
No findings |
50 |
54.9 |
47 |
51.6 |
1.00 |
||||
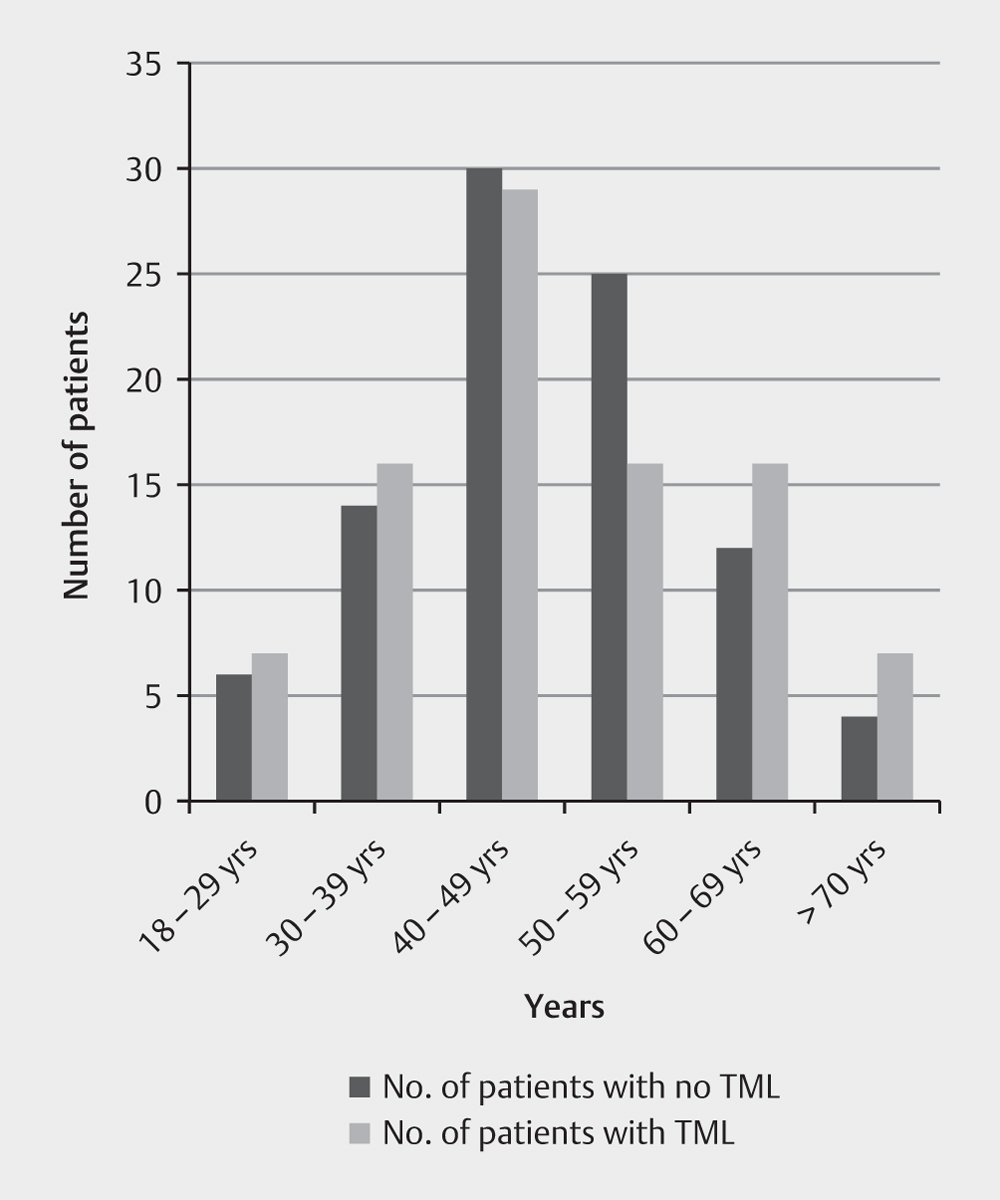
The mean testicular volume in patients with TML was 14.7 ml (range: 3.5–35.0 ml) and 14.9 ml (range: 3.0–29.9 ml) in patients without. In patients with unilateral TML, the unaffected testicles had a mean volume of 15.0 ml (range: 4.8–27.9 ml). [Table 2] shows the distribution of testicular volume. [Fig. 1] shows the distribution of patients with and without TML within a 10-year age interval. [Fig. 2] shows the mean volume in ml in the different age categories.

|
TML |
No TML |
Univariate |
Age-adjusted |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
N |
% |
N |
% |
Odds ratio |
95% CI |
P-value |
Odds ratio |
95% CI |
P-value |
|||||
|
All testicles |
182 |
100.0 |
182 |
100.0 |
||||||||||
|
Volume |
||||||||||||||
|
Median volume (ml) |
14.3 |
14.5 |
||||||||||||
|
No. of testes* with volume ≤6 |
11 |
6.0 |
7 |
3.8 |
1.61 |
0.61 |
– |
4.25 |
0.34 |
1.57 |
0.59 |
– |
4.18 |
0.36 |
|
No. of testes* with volume >6 |
171 |
94.0 |
175 |
96.2 |
1.00 |
1.00 |
||||||||
|
No. of testes* with volume ≤8 |
24 |
13.2 |
11 |
6.0 |
2.36 |
1.12 |
– |
4.98 |
0.02 |
2.34 |
1.10 |
– |
4.06 |
0.02 |
|
No. of testes* with volume >8 |
158 |
86.8 |
171 |
94.0 |
1.00 |
1.00 |
||||||||
|
No. of testes* with volume ≤10 |
40 |
22.0 |
26 |
14.3 |
1.69 |
0.98 |
– |
2.91 |
0.06 |
1.68 |
0.97 |
– |
2.89 |
0.06 |
|
No. of testes * with volume >10 |
142 |
78.0 |
156 |
85.7 |
1.00 |
1.00 |
||||||||
|
No. of testes* with volume ≤12 |
57 |
31.3 |
44 |
23.1 |
1.53 |
0.94 |
– |
2.50 |
0.08 |
1.43 |
0.90 |
– |
2.27 |
0.13 |
|
No. of testes* with volume >12 |
125 |
68.7 |
138 |
76.9 |
1.00 |
– |
– |
1.00 |
||||||
|
No. of testes* with volume ≤14 |
86 |
47.3 |
83 |
45.6 |
1.07 |
0.71 |
– |
1.61 |
0.75 |
1.08 |
0.81 |
– |
1.62 |
0.74 |
|
No. of testes* with volume >14 |
96 |
52.7 |
99 |
54.4 |
1.00 |
1.00 |
||||||||
* A total of 182 testes is eligible in each group
Discussion
The ESUR guidelines advocate yearly ultrasound follow-up examinations in patients with TML (five or more microliths per field of view) and an additional risk factor e. g. atrophic testicle [2]. A reliable and correct measurement of testicular volume is important to determine if atrophy is present. Our results showed no statistically significant difference in total testicular volume (both testicles) in patients with TML compared to patients without TML (OR 0.77 (95% CI 0.43-1.38, p=0.37). No statistically significant difference between spermatocele, hydrocele, varicocele and cyst were found in patients with TML compared to patients without TML.
The median testicular volume was 14.3 ml in patients with TML and 14.5 ml in patients without TML in this study. Von Eckardstein et al. reported a testicular volume of 13 ml in patients with unilateral TML and 15.5 ml in patients with bilateral TML [13]. In general, testicular volumes have been reported between 12–30 ml [10], and in general adult testicular volume remains stable after puberty is complete [14] [15]. Lenz et al. investigated 444 men from the general population and found a median ultrasonic volume of 14 ml in the right and 13 ml in the left testis [14]. In a later study, Lenz et al. studied the contralateral testicle in 78 patients with unilateral testicular cancer and found an ultrasonic testicular mean volume of 12.9 ml (range: 3–24 ml) [16]. In general, the reported testicular volume in patients with TML seems to be similar to patients from the general population.
Atrophy has been associated with reduced spermatogenesis and infertility, and may transpire on the basis of previous testicular inflammation, estrogen treatment, and aging [10]. Atrophy is an established risk factor for testicular cancer, and has been linked with TML [2] [13]. We found no statistically significant association between atrophy and TML, but there was a trend indicating that severe atrophy is more often seen in patients with TML compared with patients without TML (≤ 10 ml, p=0.06) and ≤ 8 ml, p=0.02). This trend is also seen in other studies, but not all have found this. One study investigated TML in 18 young boys with Down syndrome, and found testicular volume to be smaller compared to the control group [8]. Another study investigated TML in 9 young patients and found that the mean testicular volume did not differ from the control group [17]. Bayramoglu et al. investigated testicular volume in 23 pediatric patients with TML and 31 pediatric patients without TML, and found no difference in testicular volume between the study and control groups [18]. However, it is possible that ethnicity also affects testicular volume [19]. The small number of included patients may also affect the results.
In general, a difference in volume between the affected testicle and the unaffected testicle >20% is acceptable, before the diagnosis of atrophy is considered [2]. We found 46.1% of patients with TML had less than a 20% difference in volume between their two testicles. It is difficult to determine whether patients develop atrophic testes as a result of age, or as a consequence of TML, or due to other conditions. However, testicular cancer is mostly seen in young men aged 15–35 years, and in the present study TML was most frequent in patients aged 50–59 years old ([Fig. 1]). Furthermore, we found no difference in testicular volume between younger patients with and without TML (18–49 years old, [Fig. 2]). Therefore, it seems unlikely that patients with TML develop testicular atrophy as a result of age alone.
One of the strengths in this study is that scrotal ultrasound is easily performed and not a very time-consuming tool. Four investigators obtained testicular volume measurements, which limits the interobserver variation. This is confirmed in a study that showed good correlation between three investigators when measuring testicular volume [12], and ultrasound has been recognized as a reliable method. We did not use an orchidometer to measure testicular volume. On the other hand an orchidometer seems to correlate well with ultrasound measurements, even if ultrasound may slightly overestimate testicular volume [5] [20]. Another limitation is that comparison of testicular volume occurred between symptomatic patients and not between asymptomatic men from the general population. The proportion of patients with TML was high in the study population, but if the study population was e. g. twice as large, it may have been possible to show a significant difference between patients with and without TML, and not just a trend.
Conclusion
Overall, no association was found between testicular volume and TML, but there was a trend indicating that severe atrophy is often seen in patients with TML compared with patients without TML.
Conflict of Interest
The authors declare no conflict of interest.
-
References
- 1 Doherty FJ, Mullins TL, Sant GR, Drinkwater MA, Ucci AAJr. Testicular microlithiasis. A unique sonographic appearance. J Ultrasound Med 1987; 6: 389-392
- 2 Richenberg J, Belfield J, Ramchandani P, Rocher L, Freeman S, Tsili AC. et al. Testicular microlithiasis imaging and follow-up: Guidelines of the ESUR scrotal imaging subcommittee. Eur Radiol 2015; 25: 323-330
- 3 Kunde M, Kunze C, Surov A, Ruschke K, Spielmann RP. Evaluation of testicular volume in 0-18-year old boys by sonography. Urologe 2015; 54: 1772-1778
- 4 Varela-Cives R, Mendez-Gallart R, Estevez-Martinez E, Rodriguez-Barca P, Bautista-Casasnovas A, Pombo-Arias M. et al. A cross-sectional study of cryptorchidism in children: Testicular volume and hormonal function at 18 years of age. Int Braz J Urol 2015; 41: 57-66
- 5 Joustra SD, van der Plas EM, Goede J, Oostdijk W, Delemarre-van de Waal HA, Hack WW. et al. New reference charts for testicular volume in Dutch children and adolescents allow the calculation of standard deviation scores. Acta Paediatrica 2015; 104: e271-e278
- 6 Christman MS, Zderic SA, Kolon TF. Comparison of testicular volume differential calculations in adolescents with varicoceles. J Pediatr Urol 2014; 10: 396-398
- 7 Rud CN, Daugaard G, Rajpert-De Meyts E, Skakkebæk NE, Petersen JH, Jørgensen N. Sperm concentration, testicular volume and age predict risk of carcinoma in situ in contralateral testis of men with testicular germ cell cancer. J Urol 2013; 190: 2074-2080
- 8 Goede J, Weijerman ME, Broers CJ, de Winter JP, van der Voort-Doedens LM, Hack WWM. Testicular volume and testicular microlithiasis in boys with Down syndrome. J Urol 2012; 187: 1012-1017
- 9 Sakamoto H, Ogawa Y, Yoshida H. Relationship between testicular volume and testicular function: Comparison of the prader orchidometric and ultrasonographic measurements in patients with infertility. Asian J Androl 2008; 10: 319-324
- 10 Ammar T, Sidhu PS, Wilkins CJ. Male infertility: The role of imaging in diagnosis and management. Br J Radiol 2012; 85: S59-S68
- 11 Sidhu PS. Diseases of the testis and epididymis. In: Baxter GM, Sidhu Ps. editors eds. Ultrasound of the urogenrial system. Stuttgart, Germany: Thieme; 2006: 153-180 p
- 12 Goede J, Hack WWM, Sijstermans K, van der Voort-Doedens LM, Van der Ploeg T, Meij-de Vries A. et al. Normative values for testicular volume measured by ultrasonography in a normal population from infancy to adolescence. Horm Res Paediatr 2011; 76: 56-64
- 13 von Eckardstein S, Tsakmakidis G, Kamischke A, Rolf C, Nieschlag E. Sonographic testicular microlithiasis as an Indicator of premalignant conditions in normal and infertile men. J Androl 2001; 22: 818-824
- 14 Lenz S, Giwercman A, Elsborg A, Cohr KH, Jelnes JE, Carlsen E. et al. Ultrasonic testicular texture and size in 444 men from the general population: Correlation to semen quality. Eur Urol 1993; 24: 231-238
- 15 Handelsman DJ, Staraj S. Testicular size: The effects of aging, malnutrition, and illness. J Androl 1985; 6: 144-151
- 16 Lenz S, Skakkebaek NE, Hertel NT. Abnormal ultrasonic pattern in contralateral testes in patients with unilateral testicular cancer. World J Urol 1996; 14: S55-5S8
- 17 Cebeci AN, Aslanger A, Ozdemir M. Should patients with Down syndrome be screened for testicular microlithiasis?. Eur J Pediatr Surg 2015; 25: 177-180
- 18 Bayramoglu Z, Kandemirli SG, Comert RG, Akpinar YE, Caliskan E, Yilmaz R. et al. Shear wave elastography evaluation in pediatric testicular microlithiasis: A comparative study. J Med Ultrason 2018; 45: 281-286
- 19 Johnson L, Barnard JJ, Rodriguez L, Smith EC, Swerdloff RS, Wang XH. et al. Ethnic difference in testicular structure and spermatogenic potential may predispose testes of Asian men to a heightened sensitivity to steriodal contraceptives. J Androl 1998; 19: 348-357
- 20 Taskinen S, Taavitsainen M, Wikström S. Measurement of testicular volume: Comparison of 3 different methods. J Urol 1996; 155: 930-933
Correspondence
-
References
- 1 Doherty FJ, Mullins TL, Sant GR, Drinkwater MA, Ucci AAJr. Testicular microlithiasis. A unique sonographic appearance. J Ultrasound Med 1987; 6: 389-392
- 2 Richenberg J, Belfield J, Ramchandani P, Rocher L, Freeman S, Tsili AC. et al. Testicular microlithiasis imaging and follow-up: Guidelines of the ESUR scrotal imaging subcommittee. Eur Radiol 2015; 25: 323-330
- 3 Kunde M, Kunze C, Surov A, Ruschke K, Spielmann RP. Evaluation of testicular volume in 0-18-year old boys by sonography. Urologe 2015; 54: 1772-1778
- 4 Varela-Cives R, Mendez-Gallart R, Estevez-Martinez E, Rodriguez-Barca P, Bautista-Casasnovas A, Pombo-Arias M. et al. A cross-sectional study of cryptorchidism in children: Testicular volume and hormonal function at 18 years of age. Int Braz J Urol 2015; 41: 57-66
- 5 Joustra SD, van der Plas EM, Goede J, Oostdijk W, Delemarre-van de Waal HA, Hack WW. et al. New reference charts for testicular volume in Dutch children and adolescents allow the calculation of standard deviation scores. Acta Paediatrica 2015; 104: e271-e278
- 6 Christman MS, Zderic SA, Kolon TF. Comparison of testicular volume differential calculations in adolescents with varicoceles. J Pediatr Urol 2014; 10: 396-398
- 7 Rud CN, Daugaard G, Rajpert-De Meyts E, Skakkebæk NE, Petersen JH, Jørgensen N. Sperm concentration, testicular volume and age predict risk of carcinoma in situ in contralateral testis of men with testicular germ cell cancer. J Urol 2013; 190: 2074-2080
- 8 Goede J, Weijerman ME, Broers CJ, de Winter JP, van der Voort-Doedens LM, Hack WWM. Testicular volume and testicular microlithiasis in boys with Down syndrome. J Urol 2012; 187: 1012-1017
- 9 Sakamoto H, Ogawa Y, Yoshida H. Relationship between testicular volume and testicular function: Comparison of the prader orchidometric and ultrasonographic measurements in patients with infertility. Asian J Androl 2008; 10: 319-324
- 10 Ammar T, Sidhu PS, Wilkins CJ. Male infertility: The role of imaging in diagnosis and management. Br J Radiol 2012; 85: S59-S68
- 11 Sidhu PS. Diseases of the testis and epididymis. In: Baxter GM, Sidhu Ps. editors eds. Ultrasound of the urogenrial system. Stuttgart, Germany: Thieme; 2006: 153-180 p
- 12 Goede J, Hack WWM, Sijstermans K, van der Voort-Doedens LM, Van der Ploeg T, Meij-de Vries A. et al. Normative values for testicular volume measured by ultrasonography in a normal population from infancy to adolescence. Horm Res Paediatr 2011; 76: 56-64
- 13 von Eckardstein S, Tsakmakidis G, Kamischke A, Rolf C, Nieschlag E. Sonographic testicular microlithiasis as an Indicator of premalignant conditions in normal and infertile men. J Androl 2001; 22: 818-824
- 14 Lenz S, Giwercman A, Elsborg A, Cohr KH, Jelnes JE, Carlsen E. et al. Ultrasonic testicular texture and size in 444 men from the general population: Correlation to semen quality. Eur Urol 1993; 24: 231-238
- 15 Handelsman DJ, Staraj S. Testicular size: The effects of aging, malnutrition, and illness. J Androl 1985; 6: 144-151
- 16 Lenz S, Skakkebaek NE, Hertel NT. Abnormal ultrasonic pattern in contralateral testes in patients with unilateral testicular cancer. World J Urol 1996; 14: S55-5S8
- 17 Cebeci AN, Aslanger A, Ozdemir M. Should patients with Down syndrome be screened for testicular microlithiasis?. Eur J Pediatr Surg 2015; 25: 177-180
- 18 Bayramoglu Z, Kandemirli SG, Comert RG, Akpinar YE, Caliskan E, Yilmaz R. et al. Shear wave elastography evaluation in pediatric testicular microlithiasis: A comparative study. J Med Ultrason 2018; 45: 281-286
- 19 Johnson L, Barnard JJ, Rodriguez L, Smith EC, Swerdloff RS, Wang XH. et al. Ethnic difference in testicular structure and spermatogenic potential may predispose testes of Asian men to a heightened sensitivity to steriodal contraceptives. J Androl 1998; 19: 348-357
- 20 Taskinen S, Taavitsainen M, Wikström S. Measurement of testicular volume: Comparison of 3 different methods. J Urol 1996; 155: 930-933