RSS-Feed abonnieren
DOI: 10.1016/j.rbo.2018.01.001
Comparative Effect between Infiltration of Platelet-rich Plasma and the Use of Corticosteroids in the Treatment of Knee Osteoarthritis: A Prospective and Randomized Clinical Trial[*]
Artikel in mehreren Sprachen: português | English
Abstract
Objectives This study aimed to analyze the efficacy of platelet-rich plasma obtained from the peripheral, autologous blood of the patients in pain complaints reduction and functional improvement of knee osteoarthritis compared with the standard treatment with injectable corticosteroid, such as triamcinolone.
Methods The patients were followed-up clinically at the preinfiltrative visit, with quantitative evaluation using the Knee Society Score (KSS), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, and the Kellgren and Lawrence scales. In addition, they were reevaluated with the same scales after 1 month and 6 months of intervention with 2.5 mL of triamcinolone acetate or 5 mL of platelet-rich plasma. The study was performed on 50 patients with knee osteoarthritis treated at the Medical Specialty Center and randomly divided into equivalent samples for each therapy.
Results The present study verified the reduction of pain scores, such as the WOMAC score, and elevations of functional scales, such as the KSS, evidenced in 180 days when using platelet-rich plasma, a therapy that uses the autologous blood of the patient and has fewer side effects.
Conclusion Although both platelet-rich plasma and corticosteroid therapies have been shown to be effective in the reduction pain complaints and functional recovery, there was a statistically significant difference between them at 180 days. According to the results obtained, platelet-rich plasma presented longer-lasting effects within 180 days in the treatment of knee osteoarthritis.
#
Introduction
Osteoarthritis is the most common joint disease in western populations, and it mainly affects the hips, knees, hands, and feet.[1] [2] It results in progressive functional disability and several etiological factors, such as age, obesity, occupational and genetic factors, contributed to its onset.[3]
Global epidemiological studies show that the prevalence of osteoarthritis is positively associated with aging and with the female gender, with 5.3 affected women for every 3.6 affected men.[4] [5]
The loss of homeostasis between the cartilaginous matrix synthesis and degradation is the pathophysiological basis of osteoarthritis.[6] In these patients, chondrocytes and synovial cells produce high levels of proinflammatory cytokines, such as interleukin (IL)-1 and tumor necrosis factor alpha (TNF-α), which, in turn, stimulate metalloproteinases, other interleukins (IL-6, IL-8), prostaglandin E2, and nitric oxide, which is also stimulated by mechanical stress.[7]
The progression of articular chondral lesions is the main cause of nocturnal pain, stiffness, edema, and joint mobility impairment, negatively affecting the quality of life, emotional well-being (especially in the elderly), and general health status of the patient.[8]
The knees are the most commonly affected major joints, resulting in disabling symptoms that compromise the quality of life in approximately 10% of people over 55 years-old; in addition, a quarter of these patients are severely affected by immobility.[8] [9]
Several oral medications for pain relief are available and considered effective in the early stages of the disease. However, treatment should always be multifactorial, since pharmacological therapy alone is not sufficient for the desired control of osteoarthritis.[1] [9]
Infiltration treatments are usually reserved for patients with unsatisfactory response to oral regimens.[10] Hyaluronic acid infiltrations have been used for decades, but they are discouraged because of the high risk of adverse effects and irrelevant benefit when compared to intra-articular corticosteroids injections.[11] [12] As such, injectable corticosteroids are widely used in the symptomatic treatment of knee osteoarthritis; however, its efficacy appears to be limited to 1 month.[12]
Platelet-rich plasma (PRP) infiltrate is considered an emerging regenerative treatment for the osteoarthritis related-degeneration because platelet degranulation leads to the release of several growth factors and cytokines that play a crucial role in joint homeostasis.[13] Thus, it is believed that PRP promotes cellular chemotaxis, matrix synthesis, and cartilage proliferation.[14]
Although PRP has been used for the treatment of knee osteoarthritis, clinical evidence is still unclear due to the lack of standardized studies regarding the interval period, volume, and frequency of plasma infiltration.[15] [16]
The present study aimed to analyze the efficacy of PRP infiltrate, which obtained from the peripheral, autologous blood of patients, in the reduction of pain complaints and functional improvement in knee osteoarthritis when compared to the standard treatment with an injectable corticosteroid, such as triamcinolone.
#
Material and Methods
This is a randomized, controlled, longitudinal, double-blind, comparative, descriptive and analytical study of patients with knee osteoarthritis at the Unit Medical Specialty Center (Unitmed). Patients were randomized into a block, whose only specification was the equivalent number of individuals; those assigned to receive treatment with platelet-rich plasma comprised the intervention group, whereas those treated with corticosteroid injection comprised the control group.
The number of components in each sample was stipulated to achieve a 95% confidence interval, 80% power and a 20% difference between groups; as such, the intervention and group groups consisted in 25 people each, totaling 50 patients. To maintain double-blindness, peripheral blood was collected from all patients.
Platelet-rich plasma was obtained according to the double centrifugation protocol initially described by Sonnleitner et al.,[17] and validated by Messora et al.[18] In this protocol, 15 mL of peripheral blood were collected in 5 mL vacuum tubes with 3.2% sodium citrate. After the first centrifugation, the upper column was aspirated and again centrifuged, resulting in platelet-poor plasma (PPP) and a pellet of erythrocytes and platelets. Two-thirds of the PPP from the original volume were discarded, and the remaining material was used to resuspend the pellet, resulting in 5 mL of PRP for injection.
The corticosteroid used was triamcinolone acetate (Triancil, Apsen Farmacêutica, São Paulo, SP, Brazil). The infiltration was performed through intra-articular administration of 2.5 mL of the drug at a concentration of 20 mg mL, with no diluting agent.
Both infiltrations were made in the superior-lateral region of the knee operated after anesthesia with 2 mL of 2% lidocaine with no vasoconstricting agent. After the injection, the patients remained in supine position and were asked to not move the injected limb for 5 minutes.
After checking which treatment would be assigned to each patient according to the block randomization list previously generated, one of the researchers enveloped the syringe with opaque tape. This syringe was then delivered to the physician responsible for the infiltrations, and the intervention masking was maintained for both the patient and the physician.
The variables analyzed in each group were: age, gender, mean age of diagnosis, history of hypertension, obesity or diabetes, and previous orthopedic surgery in the knee analyzed.
The inclusion criteria were age ranging from 30 and 90 years-old, presence of grade II to IV osteoarthritis according to the Kellgren and Lawrence scale,[19] absence of other rheumatic inflammatory diseases, absence of previous treatment with intravenous, injectable or oral corticosteroids during the last 12 months and signature of the informed consent form.
The exclusion criteria were disease preventing follow-up, loss at follow-up, use of oral or intravenous corticosteroids during the follow-up period, hemoglobin level lower than 11 g/dL, and platelet count lower than 150,000/mm3
Therapeutic responses were evaluated using the knee society score (KSS) and the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) questionnaires, both validated and standardized for Portuguese language.[20] [21] The translated version of the KSS[20] consists in a questionnaire combining subjective and objective information about functional aspects of the patient, such as the ability to walk and climb and descend stairs, in addition to knee-associated characteristics, such as pain, stability and range of movement. KSS assesses the patient's clinical picture of pain and the degree of mobility impairment and stability in several planes. Thus, the higher the KSS score, the more clinically relevant the therapeutic response.[22] The second questionnaire, WOMAC, contains 17 questions regarding the difficulty degree in daily living activities to assess functionality, pain and stiffness. The higher the score, the worse the function.[21] [23] A possible reduction of 16% from the total WOMAC score obtained before the intervention was used as a criterion of relevant clinical difference.[24]
The patients were evaluated with these questionnaires before the procedure and at 1 month and 6 months after the infiltration. The Kellgren and Lawrence classification[19] was performed by experienced orthopedists and rheumatologists during the preinfiltrative evaluation.
This information was inserted into a database built on SPSS for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). Demographic characteristics were presented in frequencies, percentages, and respective 95% confidence intervals (95% CIs) for categorical variables and mean and standard deviation or median with 25th and 75th percentiles for continuous variables.
The mean values were compared using parametric (Student-t and analysis of variance [ANOVA] tests) or nonparametric methods (Kruskal-Wallis or Mann-Whitney) for continuous variables and chi-square for categorical variables, according to distribution type assumed by the variable. To analyze the factors associated with the outcome variable, prevalence values were determined with their respective ratios. Then, a logistic model was used to determine simple and adjusted odds ratios. The Tukey multiple comparison test was employed for therapies evaluation in the selected periods.
The level of statistical significance considered for all tests was p = 0.05 in univariate analyses. The research ensures the confidentiality and privacy of the participating professionals and assures the non-use of questionnaire information to the detriment of the people involved. The project was approved by the ethics committee and followed its recommendations.
#
Results
The 2 groups studied had the same number of individuals after random distribution, since 25 patients were assigned to each group. After inclusion in the study, there was no loss at follow-up or exclusion of patients.
In the demographic analysis of the study population, the mean ages in the PRP and corticosteroid groups were, respectively, 64.15 (±8.02) and 60.21 (±5.92) years-old (p = 0.01). From the individuals evaluated, 84% (n = 42) were females
In the present study, 90% of the patients were classified as grade II and III per the Kellgren and Lawrence scale; distribution is detailed in [Table 1].
|
Kellgren and Lawrence |
Platelet-rich plasma (%) |
Corticosteroid |
|---|---|---|
|
I |
− |
1 (4) |
|
II |
10 (40) |
10 (40) |
|
III |
11 (44) |
14 (56) |
|
IV |
4 (16) |
− |
[Table 2] shows that there is no association between comorbidities and the therapy assigned according to the selection of the groups.
|
Comorbidities |
PRP (%) |
Corticosteroid (%) |
p-value |
|---|---|---|---|
|
Obesity |
76 |
88 |
0.46 |
|
Non-obesity |
24 |
12 |
|
|
Systemic arterial hypertension |
64 |
68 |
0.76 |
|
Not hypertensive |
36 |
32 |
|
|
Diabetic |
24 |
16 |
0.48 |
|
Non-diabetic |
76 |
84 |
Regarding the evolution of the WOMAC score in the studied period, the mean value found in patients treated with corticosteroids ranged from 63.93 (ΔT = 0) to 30.06 (ΔT = 30 days) and 47.36 (ΔT = 180 days) points. Comparatively, these scores in the patients submitted to PRP therapy were 73.94 (ΔT = 0), 21.96 (ΔT = 30 days), and 32.8 (ΔT = 180 days). The pain complaint evolution can be better observed in [Figure 1].

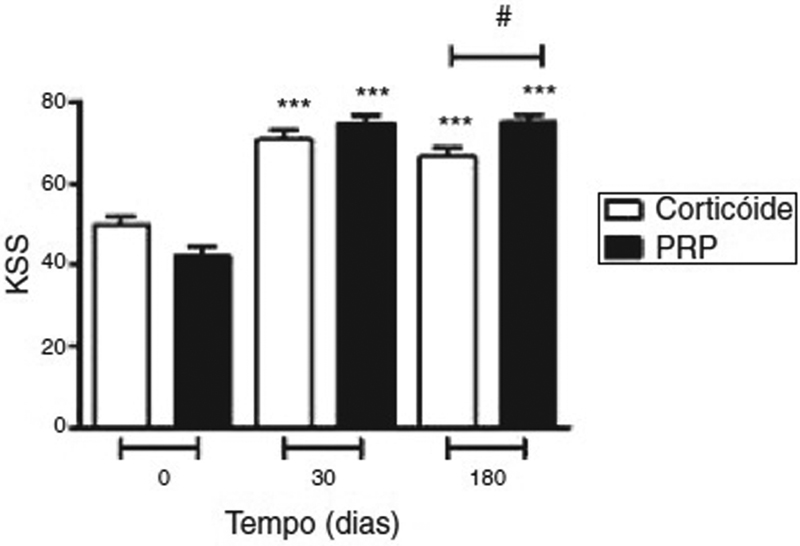
Regarding KSS, the mean values obtained in patients treated with corticosteroids were 49.96 (ΔT = 0), 70.92 (ΔT = 30 days), and 66.92 (ΔT = 180 days) points. In patients treated with PRP, the following values were found: 42.44 (ΔT = 0), 75.12 (ΔT = 30 days), and 75.36 (ΔT = 180 days) points. The evolution of the patients' functionality can be better appreciated in [Figure 2].

These results show a statistically significant difference favoring the PRP therapy at 180 days according to the WOMAC and KSS scales. On the other hand, there was no difference between study groups during the first 30 days posttreatment. Also, as shown in [Figures 1] and [2], both the corticoid and the PRP groups showed significant improvement in the WOMAC and KSS scales at 30 days and 180 days postinfiltration.
Therefore, the results obtained using PRP therapy have been shown to be more durable, with more evident functional recovery and reduction of pain complaints.
#
Discussion
Knee osteoarthritis treatment begins with a conservative approach involving a combination of analgesic agents, nonsteroidal antiinflammatory drugs (NSAIDs), and physical therapy. As the complexity of the clinical picture increases, other therapeutic methods become important, such as injectable corticosteroids, hyaluronic acid and, more recently, PRP infiltration. Patients treated with NSAIDs and analgesic agents have a better therapeutic response than those using placebo, although literature reviews consider that evidence for NSAIDs in knee osteoarthritis treatment is limited to mild to moderate cases.[25] Physical therapy, commonly performed in patients with knee osteoarthritis, is based on the ability to sustain physical fitness, flexibility and strengthening of the quadriceps muscle to aid the drug treatment.[26] Injections are used as therapies in patients who are not responsive to oral medication.[11]
Hyaluronic acid injections have been used for decades, but they have been discouraged because of the high risk of adverse effects and irrelevant benefit when compared with intra-articular corticosteroid injections. In addition, the therapeutic use of hyaluronic acid is not subsidized according to the most current recommendations and guidelines.[11] [27] As such, injectable corticosteroids are widely employed in the symptomatic treatment of knee osteoarthritis, but their efficacy appears to be limited to 1 month. Procedural repetitions may be necessary and can be performed up to 3 times a year in the same joint.[12]
Thus, the data revealed by the present study corroborate the fact that the therapeutic effect of corticosteroids is shorter (up to 30 days), while the pain improvement profile of PRP lasts up to 180 days.
Platelet-rich plasma is a constantly evolving treatment modality that has gained importance in primary care, rehabilitation, and sports medicine.[15] Since PRP is a concentrated platelet solution made with autologous blood, it is a safe treatment for clinical use.[15] Studies have shown that the intra-articular administration of PRP can increase the quality of life even after 1 year of treatment.[16] [28] The present study found more significant values for improvement in comparison with corticosteroids, especially in the long-term (180 days). Both treatments improved the functional and pain status in 30 and 180 days, but patients submitted to PRP infiltration showed a greater pain improvement in absolute numbers. In addition, there was a slight reduction in quality (5.6%) in the group receiving intra-articular corticosteroids between 30 and 180 days, although the results remained statistically more significant than in the preinfiltrative period.
The present study revealed a reduction in pain scale scores, such as the WOMAC, and an elevation in functional scale scores, such as the KSS, which were more evident in the long term (180 days) when using PRP. Although both therapies are effective and there is no significant difference between them, the results are important for the applicability of this therapeutic modality; since it is autologous, it has fewer side effects risks compared to corticosteroid infiltration with more lasting efficiency.
According to the study, 84% of the patients evaluated were elderly females.
Diabetes, hypertension, previous surgeries and obesity have been related to a higher incidence of osteoarthritis.[5] [29] [30] In our study, 66% of the patients were hypertensive and 82% were obese, corroborating the findings in the literature, but only 20% were diabetic and 2% had a history of previous surgeries.
In this study, the incidence-raising factors were homogeneous between groups regarding the therapeutic choice, demonstrating the trustworthiness of the sample and the equivalence in prior randomization.
#
Conclusion
Patients with knee osteoarthritis treated with either corticosteroid or PRP infiltration presented reduced pain complaints and increased their functionality within the first 30- and 180-days posttreatment.
However, the data presented in this study revealed that long-term (180-day) improvement rates were more significant in the PRP group.
#
#
Conflict of Interests
The authors have no conflict of interests to declare.
* Work performed at the Medical Specialty Center from Universidade Tiradentes (Unitmed), Aracaju, SE, Brazil Originally Published by Elsevier Editora Ltda.
-
Referências
- 1 Jordan KM, Arden NK, Doherty M. et al. Standing Committee for International Clinical Studies Including Therapeutic Trials ESCISIT. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003; 62 (12) 1145-1155
- 2 Lawrence RC, Felson DT, Helmick CG. et al. National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum 2008; 58 (01) 26-35
- 3 Rezende MU, De Campos GC. A osteoartrite é uma doenc¸a mecânica ou inamatória?. Rev Bras Ortop 2013; 48 (06) 471-474
- 4 Scarpone M, Rabago D, Snell E. et al. Effectiveness of platelet-rich plasma injection for rotator cuff tendinopathy: a prospective open-label study. Glob Adv Health Med 2013; 2 (02) 26-31
- 5 Pelletier JP, Martel-Pelletier J, Abramson SB. Osteoarthritis, an inflammatory disease: potential implication for the selection of new therapeutic targets. Arthritis Rheum 2001; 44 (06) 1237-1247
- 6 Fitzgerald JB, Jin M, Grodzinsky AJ. Shear and compression differentially regulate clusters of functionally related temporal transcription patterns in cartilage tissue. J Biol Chem 2006; 281 (34) 24095-24103
- 7 Sarvimäki A, Stenbock-Hult B. Quality of life in old age described as a sense of well-being, meaning and value. J Adv Nurs 2000; 32 (04) 1025-1033
- 8 Clauw DJ, Witter J. Pain and rheumatology: thinking outside the joint. Arthritis Rheum 2009; 60 (02) 321-324
- 9 Hameed F, Ihm J. Injectable medications for osteoarthritis. PM R 2012; 4 (5, Suppl): S75-S81
- 10 Evaniew N, Simunovic N, Karlsson J. Cochrane in CORR®: Viscosupplementation for the treatment of osteoarthritis of the knee. Clin Orthop Relat Res 2014; 472 (07) 2028-2034
- 11 Bannuru RR, Natov NS, Obadan IE, Price LL, Schmid CH, McAlindon TE. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Arthritis Rheum 2009; 61 (12) 1704-1711
- 12 Cheng OT, Souzdalnitski D, Vrooman B, Cheng J. Evidence-based knee injections for the management of arthritis. Pain Med 2012; 13 (06) 740-753
- 13 Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. PM R 2011; 3 (03) 226-250
- 14 Krogh TP, Bartels EM, Ellingsen T. et al. Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials. Am J Sports Med 2013; 41 (06) 1435-1446
- 15 Eppley BL, Woodell JE, Higgins J. Platelet quantification and growth factor analysis from platelet-rich plasma: implications for wound healing. Plast Reconstr Surg 2004; 114 (06) 1502-1508
- 16 Patel S, Dhillon MS, Aggarwal S, Marwaha N, Jain A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial. Am J Sports Med 2013; 41 (02) 356-364
- 17 Sonnleitner D, Huemer P, Sullivan DY. A simplified technique for producing platelet-rich plasma and platelet concentrate for intraoral bone grafting techniques: a technical note. Int J Oral Maxillofac Implants 2000; 15 (06) 879-882
- 18 Messora MR, Nagata MJ, Furlaneto FA. et al. Análise da eficiência do protocolo de dupla centrifugac¸ão para o preparo do plasma rico em plaquetas (PRP) - estudo experimental em coelhos. RSBO Rev Sul-Bras Odontol. 2009; 6 (03) 291-296
- 19 Schiphof D, Boers M, Bierma-Zeinstra SMA. Differences in descriptions of Kellgren and Lawrence grades of knee osteoarthritis. Ann Rheum Dis 2008; 67 (07) 1034-1036
- 20 Silva AL, Demange MK, Gobbi RG, da Silva TF, Pécora JR, Croci AT. Translation and Validation of the Knee Society Score - KSS for Brazilian Portuguese. Acta Ortop Bras 2012; 20 (01) 25-30
- 21 Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988; 15 (12) 1833-1840
- 22 Dinjens RN, Senden R, Heyligers IC, Grimm B. Clinimetric quality of the new 2011 Knee Society score: high validity, low completion rate. Knee 2014; 21 (03) 647-654
- 23 Oliveira AM, Peccin MS, Silva KN, Teixeira LE, Trevisani VF. Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: a randomized clinical trial. Rev Bras Reumatol 2012; 52 (06) 876-882
- 24 Hmamouchi I, Allali F, Tahiri L. et al. Clinically important improvement in the WOMAC and predictor factors for response to non-specific non-steroidal anti-inflammatory drugs in osteoarthritic patients: a prospective study. BMC Res Notes 2012; 5: 58
- 25 Eccles M, Freemantle N, Mason J. The North of England Non-Steroidal Anti-Inflammatory Drug Guideline Development Group. North of England evidence based guideline development project: summary guideline for non-steroidal anti-inflammatory drugs versus basic analgesia in treating the pain of degenerative arthritis. BMJ 1998; 317 (7157): 526-530
- 26 Roddy E, Zhang W, Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann Rheum Dis 2005; 64 (04) 544-548
- 27 Mei-Dan O, Carmont MR, Laver L, Mann G, Maffulli N, Nyska M. Platelet-rich plasma or hyaluronate in the management of osteochondral lesions of the talus. Am J Sports Med 2012; 40 (03) 534-541
- 28 Leitner GC, Gruber R, Neumüller J. et al. Platelet content and growth factor release in platelet-rich plasma: a comparison of four different systems. Vox Sang 2006; 91 (02) 135-139
- 29 Mohammadi F, Taghizadeh S, Ghaffarinejad F, Khorrami M, Sobhani S. Proprioception, dynamic balance and maximal quadriceps strength in females with knee osteoarthritis and normal control subjects. Int J Rheum Dis 2008; 11 (01) 39-44
- 30 Oliveira NC, Vatri S, Alfieri FM. Comparação dos efeitos de exercícios resistidos versus cinesioterapia na osteoartrite de joelho. Rev Acta Fisiátr. 2016; 23 (01) 7-11
Address for correspondence
Publikationsverlauf
Eingereicht: 20. Oktober 2017
Angenommen: 04. Januar 2018
Artikel online veröffentlicht:
03. Februar 2020
© 2020. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Sociedade Brasileira de Ortopedia e Traumatologia. Published by Thieme Revinter Publicações
Ltda
Rio de Janeiro, Brazil
-
Referências
- 1 Jordan KM, Arden NK, Doherty M. et al. Standing Committee for International Clinical Studies Including Therapeutic Trials ESCISIT. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003; 62 (12) 1145-1155
- 2 Lawrence RC, Felson DT, Helmick CG. et al. National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum 2008; 58 (01) 26-35
- 3 Rezende MU, De Campos GC. A osteoartrite é uma doenc¸a mecânica ou inamatória?. Rev Bras Ortop 2013; 48 (06) 471-474
- 4 Scarpone M, Rabago D, Snell E. et al. Effectiveness of platelet-rich plasma injection for rotator cuff tendinopathy: a prospective open-label study. Glob Adv Health Med 2013; 2 (02) 26-31
- 5 Pelletier JP, Martel-Pelletier J, Abramson SB. Osteoarthritis, an inflammatory disease: potential implication for the selection of new therapeutic targets. Arthritis Rheum 2001; 44 (06) 1237-1247
- 6 Fitzgerald JB, Jin M, Grodzinsky AJ. Shear and compression differentially regulate clusters of functionally related temporal transcription patterns in cartilage tissue. J Biol Chem 2006; 281 (34) 24095-24103
- 7 Sarvimäki A, Stenbock-Hult B. Quality of life in old age described as a sense of well-being, meaning and value. J Adv Nurs 2000; 32 (04) 1025-1033
- 8 Clauw DJ, Witter J. Pain and rheumatology: thinking outside the joint. Arthritis Rheum 2009; 60 (02) 321-324
- 9 Hameed F, Ihm J. Injectable medications for osteoarthritis. PM R 2012; 4 (5, Suppl): S75-S81
- 10 Evaniew N, Simunovic N, Karlsson J. Cochrane in CORR®: Viscosupplementation for the treatment of osteoarthritis of the knee. Clin Orthop Relat Res 2014; 472 (07) 2028-2034
- 11 Bannuru RR, Natov NS, Obadan IE, Price LL, Schmid CH, McAlindon TE. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Arthritis Rheum 2009; 61 (12) 1704-1711
- 12 Cheng OT, Souzdalnitski D, Vrooman B, Cheng J. Evidence-based knee injections for the management of arthritis. Pain Med 2012; 13 (06) 740-753
- 13 Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. PM R 2011; 3 (03) 226-250
- 14 Krogh TP, Bartels EM, Ellingsen T. et al. Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials. Am J Sports Med 2013; 41 (06) 1435-1446
- 15 Eppley BL, Woodell JE, Higgins J. Platelet quantification and growth factor analysis from platelet-rich plasma: implications for wound healing. Plast Reconstr Surg 2004; 114 (06) 1502-1508
- 16 Patel S, Dhillon MS, Aggarwal S, Marwaha N, Jain A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial. Am J Sports Med 2013; 41 (02) 356-364
- 17 Sonnleitner D, Huemer P, Sullivan DY. A simplified technique for producing platelet-rich plasma and platelet concentrate for intraoral bone grafting techniques: a technical note. Int J Oral Maxillofac Implants 2000; 15 (06) 879-882
- 18 Messora MR, Nagata MJ, Furlaneto FA. et al. Análise da eficiência do protocolo de dupla centrifugac¸ão para o preparo do plasma rico em plaquetas (PRP) - estudo experimental em coelhos. RSBO Rev Sul-Bras Odontol. 2009; 6 (03) 291-296
- 19 Schiphof D, Boers M, Bierma-Zeinstra SMA. Differences in descriptions of Kellgren and Lawrence grades of knee osteoarthritis. Ann Rheum Dis 2008; 67 (07) 1034-1036
- 20 Silva AL, Demange MK, Gobbi RG, da Silva TF, Pécora JR, Croci AT. Translation and Validation of the Knee Society Score - KSS for Brazilian Portuguese. Acta Ortop Bras 2012; 20 (01) 25-30
- 21 Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988; 15 (12) 1833-1840
- 22 Dinjens RN, Senden R, Heyligers IC, Grimm B. Clinimetric quality of the new 2011 Knee Society score: high validity, low completion rate. Knee 2014; 21 (03) 647-654
- 23 Oliveira AM, Peccin MS, Silva KN, Teixeira LE, Trevisani VF. Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: a randomized clinical trial. Rev Bras Reumatol 2012; 52 (06) 876-882
- 24 Hmamouchi I, Allali F, Tahiri L. et al. Clinically important improvement in the WOMAC and predictor factors for response to non-specific non-steroidal anti-inflammatory drugs in osteoarthritic patients: a prospective study. BMC Res Notes 2012; 5: 58
- 25 Eccles M, Freemantle N, Mason J. The North of England Non-Steroidal Anti-Inflammatory Drug Guideline Development Group. North of England evidence based guideline development project: summary guideline for non-steroidal anti-inflammatory drugs versus basic analgesia in treating the pain of degenerative arthritis. BMJ 1998; 317 (7157): 526-530
- 26 Roddy E, Zhang W, Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann Rheum Dis 2005; 64 (04) 544-548
- 27 Mei-Dan O, Carmont MR, Laver L, Mann G, Maffulli N, Nyska M. Platelet-rich plasma or hyaluronate in the management of osteochondral lesions of the talus. Am J Sports Med 2012; 40 (03) 534-541
- 28 Leitner GC, Gruber R, Neumüller J. et al. Platelet content and growth factor release in platelet-rich plasma: a comparison of four different systems. Vox Sang 2006; 91 (02) 135-139
- 29 Mohammadi F, Taghizadeh S, Ghaffarinejad F, Khorrami M, Sobhani S. Proprioception, dynamic balance and maximal quadriceps strength in females with knee osteoarthritis and normal control subjects. Int J Rheum Dis 2008; 11 (01) 39-44
- 30 Oliveira NC, Vatri S, Alfieri FM. Comparação dos efeitos de exercícios resistidos versus cinesioterapia na osteoartrite de joelho. Rev Acta Fisiátr. 2016; 23 (01) 7-11