RSS-Feed abonnieren
DOI: 10.1016/j.rbo.2017.12.025
Origin of the Posterior Inferior Cerebellar Artery over the C1 Posterior Arch[*]
Artikel in mehreren Sprachen: português | EnglishEndereço para correspondência
Publikationsverlauf
03. Oktober 2017
21. Dezember 2019
Publikationsdatum:
19. September 2019 (online)
Keywords
vertebral artery - cerebral angiography - anatomic variation - lateral medullary syndrome - intraoperative complicationsIntroduction
The posterior inferior cerebellar artery (PICA), or arteria inferior posterior cerebelli per Nomina Anatomica, usually arises from the intracranial segment (V4) of the vertebral artery and irrigates vital brain areas, especially the brain stem.[1] [2] Its inadvertent occlusion during surgery may cause an infarction that, although volumetrically small, produces severe and disabling sequelae.[3] An anatomical variation may predispose to iatrogenic injury even with the appropriate surgical technique.[4] We present a case of anomalous PICA arising from the cervical segment (V3) of the vertebral artery that illustrates such a possibility.
#
Case report
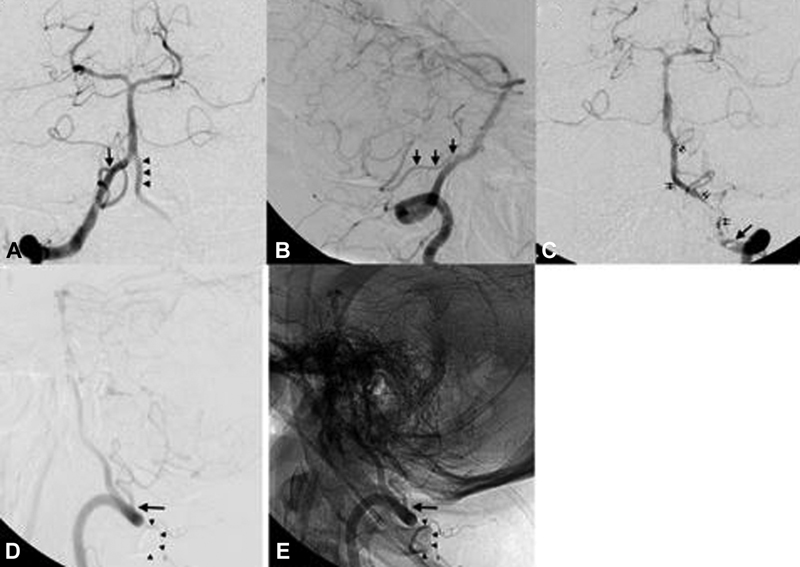
A 51-year-old male patient was admitted to the emergency department complaining of sudden onset of severe headache. He underwent a cranial tomography that showed an intracranial hemorrhage in the perimesencephalic subarachnoid space, with a suspicion of aneurysmal etiology. The patient underwent an angiography with digital subtraction of the cervical and cranial vessels that ruled out an aneurysm or arteriovenous malformation. During the angiographic examination, an anatomical variation of the left PICA was identified with an anomalous origin in the cervical segment (V3) of the ipsilateral vertebral artery ([Fig. 1]). Due to clinical improvement, the patient was discharged asymptomatic after seven days of hospitalization and a repeat angiography.

#
Discussion
The PICA can be considered the artery that irrigates the inferior posterior part of the cerebellum, but it is generally defined as the cerebellar artery arising from the vertebral artery; it is usually the largest branch of the vertebral artery, and one of the three main cerebellar nourishers.[1] [2] [4] In an anatomical study, Lister et al[1] identified the most typical origin of this artery in the V4 segment of the vertebral artery; therefore, it is intracranially and intradurally located, at an average distance of 8 mm above the foramen magnum and 17 mm below the vertebrobasilar junction.[2] [4] The PICA starts near the lower olive of the brain stem, and it surrounds and irrigates the anterior, lateral or posterior medulla oblongata through direct or circumferential perforating branches.[1] There are several descriptions for the distal PICA segment, but they are unrelated to the upper cervical instrumentation.[4] In general, after anteriorly crossing the lower cranial nerves (glossopharyngeal, vagus, accessory, and hypoglossal nerves), the PICA travels posteriorly through the cerebellar tonsils and gives branches that are distributed to the choroid plexus of the fourth ventricle, to half of the vermis, and to the suboccipital surface of the cerebellar hemisphere.[1]
The diameter of the PICA ranges from 0.5 to 3.4 mm, with an average of 2 mm.[1] However, despite its small size, its occlusion can lead to severe sequelae because this artery irrigates vital brain areas. The consequences range from clinically-silent ischemic injury to brain stem or cerebellum infarction with edema, hemorrhage, and death.[1] Virtually all PICA occlusions result in infarction, whereas approximately half of vertebral artery occlusions cause infarction, since there may be a collateral flow through the contralateral vertebral artery.[1] Occlusion of the PICA results in lateral bulb infarction, dorsal to the inferior olivary nucleus, leading to lateral bulbar syndrome, which was described in 1895 by Wallenberg[3] in a postmortem analysis. Wallenberg syndrome includes thermoanalgesia in the contralateral hemibody due to bulbar lateral spinothalamic tract injury; ipsilateral facial hemi-hypoesthesia/anesthesia due to trigeminal (V) nucleus and spinal tract injury; dysphagia and dysphonia due to ambiguous nucleus injury affecting vagus (X) and glossopharyngeal (IX) nerve functions; ipsilateral vestibular syndrome, with rotatory vertigo, diplopia, lateropulsion and nystagmus, due to vestibular nuclei injury; ipsilateral Horner syndrome due to sympathetic descending fiber injury; and ipsilateral ataxic cerebellar syndrome due to inferior cerebellar peduncle injury.[3] The PICA has the most complex, tortuous and variable course and irrigation area among the cerebellar arteries.[1] [2] The incidence of extradural PICA origin ranges from 0.7 to 20% in the literature.[2] [5] Muscle branches originating from the horizontal portion of the V3 segment of the vertebral artery, ranging from 0.2 to 0.4 mm in diameter, can be mistaken for PICA and favor the occurrence of an iatrogenic lesion.[2] Nevertheless, extradural PICA usually originates from the lateral or posterior wall of the vertebral artery and travels parallel to it, which enables its identification ([Fig. 2]).[2] In addition, it punctures the dura in contact with the vertebral artery between the atlas and the foramen magnum, but it may eventually penetrate at the C1 or C2 level.[2] The recognition of such an anatomical variation is critical in all invasive procedures at the cranial cervical transition, ranging from C1-C2 cerebrospinal fluid puncture to broader surgical approaches, such as the high cervical, lateral suboccipital and extreme lateral approaches.[2] [5]

Occipitocervical junction fixation and decompression with C1 lateral mass screws are considered safe, and are widely used.[4] The posterior arch of the atlas is often removed during the procedure, and the vertebral artery is lateralized and visible; since the medullar space is wide, there may be little concern regarding dissection. Complications, although relatively infrequent, can be catastrophic, and their risk increases in cases with anatomical variations.[4] The presence of an anatomical variation can lead to unexpected complications, as described by Nassr et al[4] in a case of pathological fracture in a patient with multiple myeloma treated with occipital-C6 fixation, including a C1 lateral mass screw. The patient presented postoperative dysarthria, imbalance and dysdiadokokinesia, and the imaging showed an infarction in the PICA territory; despite appropriate screw positioning, there was an anatomical variant with extracranial artery course around C1. A review of 29 cases of lateral bulb infarction, including PICA injury, showed symptoms of dysphagia, dysarthria, ataxia, dysmetria, dysdiadokokinesia, facial pain, vertigo, nystagmus, Horner syndrome, diplopia and myoclonus.[6] Although not all symptoms are perfectly correlated with classical lateral bulbar syndrome, the diagnosis requires a high index of suspicion because the neurophysiological monitoring may not show any intraoperative change.[4] In another recent systematic literature review, Akinduro et al[7] found an incidence of 2.9% of vascular lesions during posterior atlantoaxial instrumentation, 10% of which resulted in ipsilateral infarction, and 6.7% led to death. The endovascular treatment was performed in 13.3% of the cases, and resulted in repair of the lesion without permanent deficits.
Preoperative knowledge of anatomical variations may affect surgical planning and prevent vascular complications.[4] The largest study on the abnormal origin of the PICA below the posterior arch of the atlas showed an incidence of 1% after an analysis of 346 angiograms, and it was performed after a case of PICA injury during a C1-C2 puncture.[8] Multiple variations of the vertebrobasilar system have been described and related to increased risk in high cervical surgeries.[4] Vertebral ectasia may be secondary to atherosclerosis dilation or congenital malformation,[9] and the perforation of the dura in the interlaminar space may result in mass effect.[4] Therefore, occipital neuralgia symptoms, including pulsatile headache and foramen enlargement, should raise the suspicion of an anatomical variation.[10] In the most common variation, the vertebral artery rises laterally after leaving the C2 transverse foramen, and it enters the bony canal created between the atlas and the occipital bone.[4] The next variation occurs when the vertebral artery enters the medullary canal below the posterior arch of C1 and crosses the lateral mass surface.[4] Finally, surgical complications may be caused by the presence of a proatlantal artery, which is persistent in embryonic carotid basilar anastomoses.[4] This artery joins the vertebral artery at the C1-C2 level to enter the foramen magnum; this variation is usually associated with ipsilateral vertebral artery hypoplasia or agenesis.[4] Tokuda et al,[5] after studying the angiographies of 300 patients, found 2 cases of vertebral artery penetrating the dura below C1, 3 cases of vertebral artery duplication, and 2 cases of PICA originating in C2. Wang et al[11] investigated 36 patients diagnosed with occipitalization of the atlas, and showed that 86% of the arteries would be at risk of iatrogenic injury during screw placement in C1.
The indication of preoperative vascular imaging is still a matter of debate, but angiotomography enables the assessment of the location of the arteries.[4] There will be no carotid injury if the anterior surface of the C1 lateral mass is not drilled or crossed by a guidewire, or if the screw is implanted unicortically.[4] However, some anatomical variations, including aberrant PICA and proatlantal artery, can only be diverted to avoid injury if the change is previously known.[4] Although the incidence of vertebral vascular anomalies is unknown in the general population, a series of 300 angiograms found an incidence of 3%.[5] Possible indications for vascular imaging before surgery include occipital neuralgia symptoms and congenital bone anomalies at the craniocervical region, such as occipitalization of the atlas.[11] Nassr et al,[4] however, indicate routine preoperative angiotomography for the planning of upper cervical instrumentation, especially in C1.[4] Ultimately, since the surgeon is responsible for procedural complications, he/she must decide which tests should be performed before surgery.[4]
This anatomical variation highlights the importance of the careful dissection of the C1 arch before its removal, as well as of the care required for the coagulation and dissection of the vessels in this region. In cases of vascular injury, some patients may benefit from the endovascular treatment. Knowledge of the vascular anatomy of the normal cranial cervical transition and its variations enables an accurate topographic diagnosis and proper surgical planning, minimizes complications, and improves the therapeutic outcomes.
#
#
Conflitos de Interesse
Os autores declaram não haver conflitos de interesse.
* Work developed at Hospital Universitário Cajuru, Pontifícia Universidade Católica do Paraná (PUC-PR), Curitiba, PR, Brazil. Originally published by Elsevier.
-
Referências
- 1 Lister JR, Rhoton Jr AL, Matsushima T, Peace DA. Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 1982; 10 (02) 170-199
- 2 Fine AD, Cardoso A, Rhoton Jr AL. Microsurgical anatomy of the extracranial-extradural origin of the posterior inferior cerebellar artery. J Neurosurg 1999; 91 (04) 645-652
- 3 Wallenberg A. Akute Bulbäraffektion (Embolie der Arteria cerebelli post inf sinistra). Archives fur Psychiatry 1895; 27: 504-540
- 4 Nassr AN, Swann PP, Huston III J, Abdelfatah MM, Rose PS, Currier BL. Aberrant posterior inferior cerebellar artery injury with C1 lateral mass screw placement: a case report and review of the literature. Spine J 2014; 14 (09) e7-e14
- 5 Tokuda K, Miyasaka K, Abe H. , et al. Anomalous atlantoaxial portions of vertebral and posterior inferior cerebellar arteries. Neuroradiology 1985; 27 (05) 410-413
- 6 Fukuoka T, Takeda H, Dembo T. , et al. Clinical review of 37 patients with medullary infarction. J Stroke Cerebrovasc Dis 2012; 21 (07) 594-599
- 7 Akinduro OO, Baum GR, Howard BM. , et al. Neurological outcomes following iatrogenic vascular injury during posterior atlanto-axial instrumentation. Clin Neurol Neurosurg 2016; 150: 110-116
- 8 Brinjikji W, Cloft H, Kallmes DF. Anatomy of the posterior inferior cerebellar artery: relevance for C1-C2 puncture procedures. Clin Anat 2009; 22 (03) 319-323
- 9 Vincentelli F, Caruso G, Rabehanta PB, Rey M. Surgical treatment of a rare congenital anomaly of the vertebral artery: case report and review of the literature. Neurosurgery 1991; 28 (03) 416-420
- 10 Sharma RR, Parekh HC, Prabhu S, Gurusinghe NT, Bertolis G. Compression of the C-2 root by a rare anomalous ectatic vertebral artery. Case report. J Neurosurg 1993; 78 (04) 669-672
- 11 Wang S, Wang C, Liu Y, Yan M, Zhou H. Anomalous vertebral artery in craniovertebral junction with occipitalization of the atlas. Spine 2009; 34 (26) 2838-2842
Endereço para correspondência
-
Referências
- 1 Lister JR, Rhoton Jr AL, Matsushima T, Peace DA. Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 1982; 10 (02) 170-199
- 2 Fine AD, Cardoso A, Rhoton Jr AL. Microsurgical anatomy of the extracranial-extradural origin of the posterior inferior cerebellar artery. J Neurosurg 1999; 91 (04) 645-652
- 3 Wallenberg A. Akute Bulbäraffektion (Embolie der Arteria cerebelli post inf sinistra). Archives fur Psychiatry 1895; 27: 504-540
- 4 Nassr AN, Swann PP, Huston III J, Abdelfatah MM, Rose PS, Currier BL. Aberrant posterior inferior cerebellar artery injury with C1 lateral mass screw placement: a case report and review of the literature. Spine J 2014; 14 (09) e7-e14
- 5 Tokuda K, Miyasaka K, Abe H. , et al. Anomalous atlantoaxial portions of vertebral and posterior inferior cerebellar arteries. Neuroradiology 1985; 27 (05) 410-413
- 6 Fukuoka T, Takeda H, Dembo T. , et al. Clinical review of 37 patients with medullary infarction. J Stroke Cerebrovasc Dis 2012; 21 (07) 594-599
- 7 Akinduro OO, Baum GR, Howard BM. , et al. Neurological outcomes following iatrogenic vascular injury during posterior atlanto-axial instrumentation. Clin Neurol Neurosurg 2016; 150: 110-116
- 8 Brinjikji W, Cloft H, Kallmes DF. Anatomy of the posterior inferior cerebellar artery: relevance for C1-C2 puncture procedures. Clin Anat 2009; 22 (03) 319-323
- 9 Vincentelli F, Caruso G, Rabehanta PB, Rey M. Surgical treatment of a rare congenital anomaly of the vertebral artery: case report and review of the literature. Neurosurgery 1991; 28 (03) 416-420
- 10 Sharma RR, Parekh HC, Prabhu S, Gurusinghe NT, Bertolis G. Compression of the C-2 root by a rare anomalous ectatic vertebral artery. Case report. J Neurosurg 1993; 78 (04) 669-672
- 11 Wang S, Wang C, Liu Y, Yan M, Zhou H. Anomalous vertebral artery in craniovertebral junction with occipitalization of the atlas. Spine 2009; 34 (26) 2838-2842