Subscribe to RSS
DOI: 10.1016/j.rbo.2017.09.011
Development of a Patient-specific Guide for High Cervical Spine Fixation[*]
Article in several languages: português | EnglishAddress for correspondence
Publication History
16 August 2017
05 September 2017
Publication Date:
01 March 2019 (online)
Abstract
Objective
High cervical spine fixation represents a challenge for spine surgeons due to the complex anatomy and the risks of vascular and medullar injury. The recent advances in 3-D printing have unfolded a whole new range of options for these surgeons.
Methods
In the present study, a guide for the placement of the lateral mass screw in the C1 vertebra was developed using 3-D printing. Eight real-size models of the high cervical spine and their respective screw guides were built using computed tomography (CT) scan images. The guidewires were inserted with the help of the printed guides and then the models were analyzed with the help of CT scan images.
Results
All of the guidewires in the present study obtained a safe placement in the models, avoiding the superior and inferior articular surfaces, the vertebral foramen, and the vertebral artery.
Conclusion
The present study demonstrated the efficiency of the guide, a reliable tool for aiding the insertion of guidewires for screws in lateral masses of the C1.
#
Keywords
cervical vertebrae/pathology - cervical vertebrae/surgery - spinal fractures - spinal fusion - three-dimensional printingIntroduction
High cervical spine fixation always challenges spine surgeons. The complex anatomy, the importance of this region to cervical mobility,[1] and the relatively small area for fixation result in several technical difficulties.[2] Initially, the fixation methods were insufficient, as the fusion techniques from Brooks-Jenkins or Gallie,[3] and required prolonged external fixation, or they were extensive, included the occipital region, and significantly limited the mobility of the high cervical spine.
The introduction of the screw fixation at the lateral masses, initially with Goel et al[4] and then with Harms et al,[5] changed the surgical spectrum for high cervical spine. However, the anatomical challenges persisted, mainly due to the location of the vertebral artery, which is lateral and superior to the entrance point of the screws,[6] anterior to the carotid artery, medial to the spinal cord,[7] and to the extensive venous plexus adjacent to the root of the C2 vertebra at the screw entrance point in the C1 vertebra.[2] Moreover, this procedure requires continuous radioscopy, which is harmful both to the patient and to the medical team.[8]
The use of computed navigation emerged as an option to increase the accuracy of this method.[9] However, its cost is elevated, and this technique is not available in most hospitals.
In the present study, the authors aimed to provide a low cost, easy-access option to reduce the risks associated with high cervical fixation using a guide specific for the anatomy of the patient, developed with 3-D printing.
The objective was to evaluate the accuracy of the fixation of the lateral masses of the C1 vertebra with a patient-specific guide made with a 3-D printer from a 3-D cervical model built from control computed tomography (CT) scans.
#
Material and Methods
Population
The population of the present study consists of unidentified CT images from 8 adult patients > 18 years old. None of the eight patients presented extreme morphological alterations or significant deformities at the high cervical spine.
#
Radiological Technique
High-resolution, thin-slice CT scans (01 mm) were selected. The films were analyzed by the authors, who determined the absence of important deformities and the presence of preserved, significant anatomical landmarks.
#
Preparation of the High Cervical Spine Models
Using the InVesalius software (CTI, Campinas, SP, Brazil), sequential two-dimensional CT images were converted in a 3-D model, which was then exported to CAD 3D Meshmixer (Autodesk Inc., San Rafael, CA, United States) and operated to isolate the C1 and C2 vertebrae, and a part of the C3 vertebra.
Cervical vertebrae models were printed in acrylonitrile butadiene styrene (ABS) with a 3-D Vantage I printer (Stratasys Inc., Eden Prairie, MN, United States) in a 1:1 scale ([Fig. 1]).

#
Preparation of the Pedicle Fixation Guides
With the cervical spine models ready, a guide for pedicle screws was created. These guides were designed for stable adapting over the vertebrae, limiting the lateral or superior-inferior translation and trying to avoid anatomically important structures.
Using the CAD 3D Meshmixer software (Autodesk Inc., San Rafael, CA, USA), the virtual model of the guide was then assembled over each individual high cervical virtual reconstruction. A Boolean operation identified the intersection between the models and fine adjustments were individually performed for the proper fitting of the guides at the posterior surfaces of all of the evaluated cervical spines.
Each guide path was individually defined with the help of a surgeon, simulating on the computer the desired track for each screw.
The guide models were then printed in acrylic resin Fullcure 720 with an Objet EDEN250 printer (Stratasys, Eden Prairie, MN, USA) ([Fig. 2]).

#
Adaptation of the Guidewires
The printed guides were adapted over their respective printed cervical spine models. The cervical models fit perfectly to the guides, which were stable at handling.
With the models firmly secured with a bench vise, and with the guides adapted and firmly positioned by the surgeon, both pedicles from the eight C1 vertebrae were perforated with a 1.5 mm drill. After the perforation, the drill was released from the equipment and remained fixed to the model.
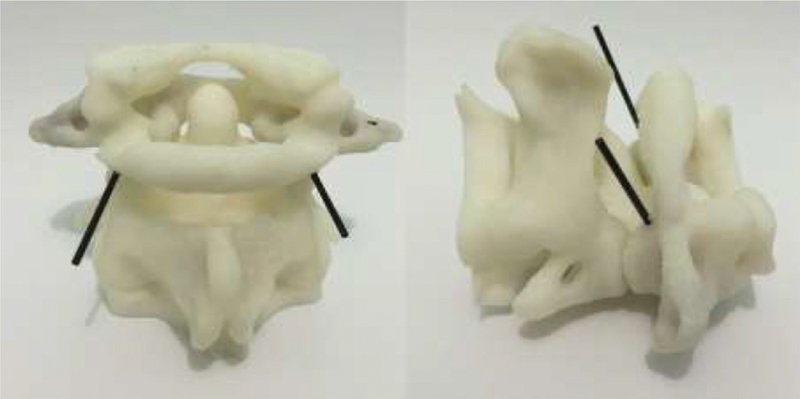
After performing the 16 perforations, the guides were removed, and the parts were sent to a diagnostic imaging facility for the thin-slice (01 mm) CT scan ([Figs. 3]–[4]).


#
Analysis of the Results
After imaging the parts with the adapted guidewires, their position was measured by the RadiAnt DICOM Viewer software (Medixant, Poznan, Poland) based on four parameters: distance from the guidewire to the vertebral artery foramen; distance from the guidewire to the medullary canal; distance from the guidewire to the superior articular surface of the C1 vertebra; and distance from the guidewire to inferior articular surface of the C1 vertebra ([Fig. 5]).

#
#
Results
The CT scan images showed that none of the 16 guidewires from the 8 models invaded the medullary canal area or the articular surfaces, neither were at the region of the vertebral artery path.
The distance from the vertebral artery foramen ranged from 2.8 to 6.2 mm, with a mean value of 4.08 mm, a median value of 4 mm, and a standard deviation (SD) of 0.937 mm.
The distance from the vertebral canal ranged from 3.7 to 8 mm, with a mean value of 5.83 mm, a median value of 6 mm, and a SD of 1.266 mm.
The distance from the guidewire to the superior articular surface of the C1 vertebra ranged from 5.9 to 10.7 mm, with a mean value of 7.52 mm, a median value of 7.1 mm, and a SD of 1.212 mm.
The distance from the guidewire to the inferior articular surface of the C1 ranged from 2.0 to 5.9 mm, with a mean value of 3.62 mm, a median value of 3.5 mm, and a SD of 0.988 mm.
The values for each parameter are listed in [Table 1].
|
Model 01 |
Model 02 |
Model 03 |
Model 04 |
Model 05 |
Model 06 |
Model 07 |
Model 08 |
|
|---|---|---|---|---|---|---|---|---|
|
DCVD |
6.1 |
6.6 |
7.4 |
3.7 |
8 |
6.1 |
5.4 |
5.1 |
|
DCVE |
5.1 |
6.3 |
4.5 |
3.8 |
7.7 |
6.0 |
6.4 |
5.2 |
|
DAVD |
4.4 |
3.4 |
3.0 |
3.5 |
2.8 |
3.6 |
4.0 |
4.2 |
|
DAVE |
5.1 |
3.3 |
6.2 |
5.7 |
4.2 |
4.4 |
3.5 |
4.0 |
|
DSASD |
6.7 |
5.9 |
8.3 |
6.6 |
10.7 |
4.4 |
7.0 |
7.7 |
|
DSASE |
7.2 |
6.8 |
8.6 |
6.7 |
9.2 |
4.0 |
6.6 |
7.6 |
|
DSAID |
4.0 |
3.2 |
4.2 |
2.0 |
2.8 |
7.8 |
2.6 |
5.1 |
|
DSAIE |
3.0 |
3.0 |
3.9 |
3.0 |
3.8 |
8.0 |
3.1 |
5.9 |
#
Discussion
Three-dimensional printing became a promising resource to help planning and executing complex spinal surgeries, allowing to recreate, with great accuracy, intricate anatomical models from imaging results.[10] [11] [12]
This technique is already successful in anatomic studies and surgical planning, as well as in the creation of biocompatible implants.[13] [14] [15]
Recent studies investigate the efficacy of 3-D printing in preparing patient-specific surgical guides to assist the adaptation of pedicle screws in lumbar and thoracic spine vertebrae. Moreover, there is evidence of good results with the intraoperative in vivo use of these guides.
In an experiment by Fu et al,[16] polymethyl methacrylate guides for transpedicle screws were manually molded over cervical vertebrae models prepared with a 3-D printer and tested in cadaveric vertebrae, with good results and easy applicability.
Some studies have also tried to develop pedicle screw guides for cervical vertebrae printed directly in 3-D, with excellent results. In an experiment by Sugawara et al,[17] 100% of 80 adapted screws in 20 patients were precisely located according to the preoperative planned path, with an average deviation of 0.29 ± 0.31 mm (0.0 mm–1.6 mm).
Studies regarding 3-D printing in vertebral spine surgery are still scarce and, until now, there is not a consistent study about these pedicle guides for the C1 vertebra in the literature.
The atlantoaxial region is a surgical challenge with unique anatomical and biomechanical properties. Several techniques were developed, but the fixation of screws in the lateral mass of the C1 vertebra gained prominence during the last decade.[18]
There are technical difficulties to identify and access the optimal entrance point for the lateral mass screw in the C1 vertebra. For this reason, a careful preoperative planning is required to avoid the bad positioning of the screws and the excessive exposure that can cause expressive bleeding and harm the success of the surgery.[18] [19]
Difficulties during the approach to the posterior aspect of the lateral mass of the C1 vertebra include abundant bleeding when exposing the inferior aspect of the posterior arch and the posterior portion of the lateral mass of the C1 vertebra,[20] and the risk of vertebral artery lesion when mobilizing it in the groove of the arch of the C1 vertebra.[6]
The exposition of the nerve of the C2 vertebra and the careful dissection of the tissues adjacent to the dorsal ganglion of the root of the C2 vertebra should be performed.[6]
The screws are directly inserted in the lateral mass of the C1 vertebra, inferiorly to the base of the posterior arch. The dimensions of the lateral mass of the C1 vertebra easily accommodate 3.5 mm screws in most patients.[19]
According to a technique described by Harms et al,[5] the screws must be inserted in a posterior-anterior direction, with 5° to 10° of convergence on the axial plane. At the sagittal plane, they must remain parallel to the caudal aspect of the posterior arch of the C1 vertebra, pointing to the center of the anterior tubercle of the C1 vertebra.[6]
During the studies to prepare these guides through computer-modeling, these anatomical aspects were carefully noted to define an individual, optimal path for each model.
The originality of the present study created some difficulties regarding the optimal format of the guide. Different guide models were prepared and tested to determine which one would present the highest stability when adapted to their respective vertebral models.
Analyzing the number figures for each vertebra, anatomical differences in morphology and size between the eight models were considered.
The guidewires did not invade the joint region, the medullary canal or the vertebral artery path of none of the eight models. All of the 16 guidewires were passed only once, with no false trajectories.
All of the adapted guidewires satisfactorily kept their paths through the center of the lateral masses of the C1 vertebra and presented enough adjacent bone mass for a possible adaptation of a cannulated screw in a safe manner.
The guides were resistant to drilling, and there was no printed guide rupture or material deformity due to the heat generated by the burr. A small amount of debris originated from the guides was observed after drilling. Since the current literature lacks conclusive data about the long-term effect of this debris in living organisms, additional studies are warranted.
Due to the good results obtained with the guides, new studies will be performed to improve the guides and verify their possible in vivo applicability.
#
Conclusion
The experiment showed that patient-specific guides made with a 3-D printer allowed the positioning of guidewires in the lateral mass of the C1 vertebra with a precision of 100%. These guides are easily applied, can benefit the adaptation of the screws in the lateral mass of the C1 vertebra, and provide a safe path for the screws.
#
#
Conflitos de Interesse
Os autores declaram não haver conflitos de interesse.
* Work developed at the Hospital Universitário Cajuru, Curitiba, PR, Brazil.
-
Referências
- 1 Swartz EE, Floyd RT, Cendoma M. Cervical spine functional anatomy and the biomechanics of injury due to compressive loading. J Athl Train 2005; 40 (03) 155-61
- 2 Abumi K, Shono Y, Ito M, Taneichi H, Kotani Y, Kaneda K. Complications of pedicle screw fixation in reconstructive surgery of the cervical spine. Spine 2000; 25 (08) 962-9
- 3 Mummaneni PV, Haid RW. Atlantoaxial fixation: overview of all techniques. Neurol India 2005; 53 (04) 408-15
- 4 Goel A, Laheri V. Plate and screw fixation for atlanto-axial subluxation. Acta Neurochir (Wien) 1994; 129 (1-2): 47-53
- 5 Goel A, Laheri V. Re: Harms J, Melcher P. Posterior C1-C2 fusion with polyaxial screw and rod fixation. (Spine 2001;26: 2467-71). Spine 2002; 27 (14) 1589-90
- 6 Schulz R, Macchiavello N, Fernández E, Carredano X, Garrido O, Diaz J. , et al. Harms C1-C2 instrumentation technique: anatomo-surgical guide. Spine 2011; 36 (12) 945-50
- 7 Currier BL, Maus TP, Eck JC, Larson DR, Yaszemski MJ. Relationship of the internal carotid artery to the anterior aspect of the C1 vertebra: implications for C1-C2 transarticular and C1 lateral mass fixation. Spine 2008; 33 (06) 635-9
- 8 Mettler Jr FA, Koenig TR, Wagner LK, Kelsey CA. Radiation injuries after fluoroscopic procedures. Semin Ultrasound CT MR 2002; 23 (05) 428-42
- 9 Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar, and sacral spine. Spine 2000; 25 (05) 606-14
- 10 Wu AM, Shao ZX, Wang JS, Yang XD, Weng WQ, Wang XY. , et al. The accuracy of a method for printing three-dimensional spinal models. PLoS One 2015; 10 (04) e0124291
- 11 Yang M, Li C, Li Y, Zhao Y, Wei X, Zhang G. , et al. Application of 3D rapid prototyping technology in posterior corrective surgery for Lenke 1 adolescent idiopathic scoliosis patients. Medicine (Baltimore) 2015; 94 (08) e582
- 12 Mizutani J, Matsubara T, Fukuoka M, Tanaka N, Iguchi H, Furuya A. , et al. Application of full-scale three-dimensional models in patients with rheumatoid cervical spine. Eur Spine J 2008; 17 (05) 644-9
- 13 Whatley BR, Kuo J, Shuai C, Damon BJ, Wen X. Fabrication of a biomimetic elastic intervertebral disk scaffold using additive manufacturing. Biofabrication 2011; 3 (01) 015004
- 14 Xu N, Wei F, Liu X, Jiang L, Cai H, Li Z. , et al. Reconstruction of the upper cervical spine using a personalized 3D-printed vertebral body in an adolescent with Ewing sarcoma. Spine 2016; 41 (01) E50-4
- 15 Wu AM, Wang S, Weng WQ, Shao ZX, Yang XD, Wang JS. , et al. The radiological feature of anterior occiput-to-axis screw fixation as it guides the screw trajectory on 3D printed models: a feasibility study on 3D images and 3D printed models. Medicine (Baltimore) 2014; 93 (28) e242
- 16 Fu M, Lin L, Kong X, Zhao W, Tang L, Li J. , et al. Construction and accuracy assessment of patient-specific biocompatible drill template for cervical anterior transpedicular screw (ATPS) insertion: an in vitro study. PLoS One 2013; 8 (01) e53580
- 17 Sugawara T, Higashiyama N, Kaneyama S, Takabatake M, Watanabe N, Uchida F. , et al. Multistep pedicle screw insertion procedure with patient-specific lamina fit-and-lock templates for the thoracic spine: clinical article. J Neurosurg Spine 2013; 19 (02) 185-90
- 18 Wang MY, Samudrala S. Cadaveric morphometric analysis for atlantal lateral mass screw placement. Neurosurgery 2004; 54 (06) 1436-9 , discussion 1439–40
- 19 Ma XY, Yin QS, Wu ZH, Xia H, Liu JF, Zhong SZ. Anatomic considerations for the pedicle screw placement in the first cervical vertebra. Spine 2005; 30 (13) 1519-23
- 20 Christensen DM, Eastlack RK, Lynch JJ, Yaszemski MJ, Currier BL. C1 anatomy and dimensions relative to lateral mass screw placement. Spine 2007; 32 (08) 844-8
Address for correspondence
-
Referências
- 1 Swartz EE, Floyd RT, Cendoma M. Cervical spine functional anatomy and the biomechanics of injury due to compressive loading. J Athl Train 2005; 40 (03) 155-61
- 2 Abumi K, Shono Y, Ito M, Taneichi H, Kotani Y, Kaneda K. Complications of pedicle screw fixation in reconstructive surgery of the cervical spine. Spine 2000; 25 (08) 962-9
- 3 Mummaneni PV, Haid RW. Atlantoaxial fixation: overview of all techniques. Neurol India 2005; 53 (04) 408-15
- 4 Goel A, Laheri V. Plate and screw fixation for atlanto-axial subluxation. Acta Neurochir (Wien) 1994; 129 (1-2): 47-53
- 5 Goel A, Laheri V. Re: Harms J, Melcher P. Posterior C1-C2 fusion with polyaxial screw and rod fixation. (Spine 2001;26: 2467-71). Spine 2002; 27 (14) 1589-90
- 6 Schulz R, Macchiavello N, Fernández E, Carredano X, Garrido O, Diaz J. , et al. Harms C1-C2 instrumentation technique: anatomo-surgical guide. Spine 2011; 36 (12) 945-50
- 7 Currier BL, Maus TP, Eck JC, Larson DR, Yaszemski MJ. Relationship of the internal carotid artery to the anterior aspect of the C1 vertebra: implications for C1-C2 transarticular and C1 lateral mass fixation. Spine 2008; 33 (06) 635-9
- 8 Mettler Jr FA, Koenig TR, Wagner LK, Kelsey CA. Radiation injuries after fluoroscopic procedures. Semin Ultrasound CT MR 2002; 23 (05) 428-42
- 9 Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar, and sacral spine. Spine 2000; 25 (05) 606-14
- 10 Wu AM, Shao ZX, Wang JS, Yang XD, Weng WQ, Wang XY. , et al. The accuracy of a method for printing three-dimensional spinal models. PLoS One 2015; 10 (04) e0124291
- 11 Yang M, Li C, Li Y, Zhao Y, Wei X, Zhang G. , et al. Application of 3D rapid prototyping technology in posterior corrective surgery for Lenke 1 adolescent idiopathic scoliosis patients. Medicine (Baltimore) 2015; 94 (08) e582
- 12 Mizutani J, Matsubara T, Fukuoka M, Tanaka N, Iguchi H, Furuya A. , et al. Application of full-scale three-dimensional models in patients with rheumatoid cervical spine. Eur Spine J 2008; 17 (05) 644-9
- 13 Whatley BR, Kuo J, Shuai C, Damon BJ, Wen X. Fabrication of a biomimetic elastic intervertebral disk scaffold using additive manufacturing. Biofabrication 2011; 3 (01) 015004
- 14 Xu N, Wei F, Liu X, Jiang L, Cai H, Li Z. , et al. Reconstruction of the upper cervical spine using a personalized 3D-printed vertebral body in an adolescent with Ewing sarcoma. Spine 2016; 41 (01) E50-4
- 15 Wu AM, Wang S, Weng WQ, Shao ZX, Yang XD, Wang JS. , et al. The radiological feature of anterior occiput-to-axis screw fixation as it guides the screw trajectory on 3D printed models: a feasibility study on 3D images and 3D printed models. Medicine (Baltimore) 2014; 93 (28) e242
- 16 Fu M, Lin L, Kong X, Zhao W, Tang L, Li J. , et al. Construction and accuracy assessment of patient-specific biocompatible drill template for cervical anterior transpedicular screw (ATPS) insertion: an in vitro study. PLoS One 2013; 8 (01) e53580
- 17 Sugawara T, Higashiyama N, Kaneyama S, Takabatake M, Watanabe N, Uchida F. , et al. Multistep pedicle screw insertion procedure with patient-specific lamina fit-and-lock templates for the thoracic spine: clinical article. J Neurosurg Spine 2013; 19 (02) 185-90
- 18 Wang MY, Samudrala S. Cadaveric morphometric analysis for atlantal lateral mass screw placement. Neurosurgery 2004; 54 (06) 1436-9 , discussion 1439–40
- 19 Ma XY, Yin QS, Wu ZH, Xia H, Liu JF, Zhong SZ. Anatomic considerations for the pedicle screw placement in the first cervical vertebra. Spine 2005; 30 (13) 1519-23
- 20 Christensen DM, Eastlack RK, Lynch JJ, Yaszemski MJ, Currier BL. C1 anatomy and dimensions relative to lateral mass screw placement. Spine 2007; 32 (08) 844-8