Subscribe to RSS
DOI: 10.1055/s-0037-1600870
Transclival Approach, Clipping and Drainage of a Giant Vertebrobasilar Aneurysm: Case Report
Publication History
Publication Date:
02 March 2017 (online)

Introduction: Transclival approach for clipping vertebrobasilar junction aneurysms has been described since 1966; however, there is not register in the current literature using this approach for clipping and drainage of giant vertebrobasilar aneurysms, mainly because its inherent complications. Approach is intended to avoid brainstem and cranial nerves retraction. Endovascular treatment has not provide enough satisfactory results concerning to brainstem decompression.
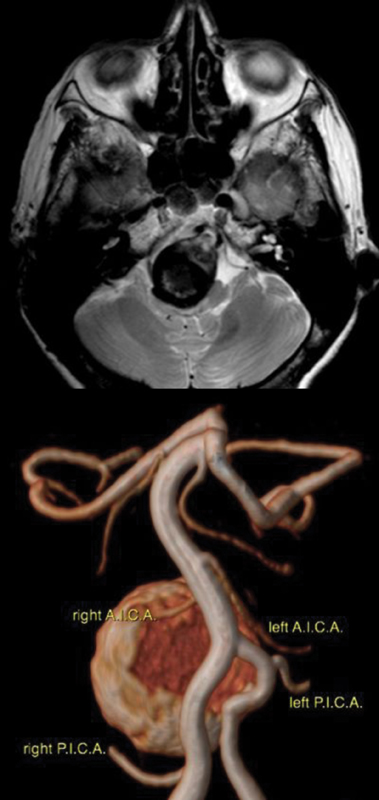
Case Report: An 84-year-old female patient, background of intense tabaquism since her 20s, arterial hypertension, and pulmonary emphysema. Her symptoms were first noticed in 2004 characterized by occasional numbness of the limbs and headache, with MRI evidence of a giant vertebrobasilar aneurysm which caused brainstem compression. At that time, neurosurgeon-determined treatment was not necessary. I met the patient on November 2014, clinically unable to swallow and unable to perform verbal communication; affection of bilateral IX, X, XI, and XII cranial nerves; hyperreflexia; and limbs strength diminished making ambulation impossible. Karnofsky was 40%.
MRI and angio-MRI showed severe brainstem compression secondary to a partially thrombosed giant vertebrobasilar aneurysm.
After detailed preoperative examination, surgery was performed under general intravenous anesthesia, sublabial mucosa was incised, LeFort I maxillotomy and sphenoidectomy was completed, clivus was high-speed drilled, dura was K-shape opened, vertebral arteries were dissected to their vertebrobasilar junction where aneurysmal neck was identified and dissected. Aneurysm clip (45-degree angulated fenestrated clip) was placed around right vertebral artery closing aneurysmal neck in left vertebrobasilar junction.
Once clip was placed, pseudo-capsule was opened and debulked with ultrasonic aspiration. Dura was partially closed, epidural fat and fascia lata graft were placed and sealed with fibrin product.
First week postoperative, the patient recovered swallowing, verbal communication, and strength. At the second postoperative week she was able to stand, and walking started at the third week.
Discussion: Transclival approach for clipping vertebrobasilar complex aneurysm has been described by Sano and others, however aneurysms were not causing brainstem compression. The principal complications are CSF leak and meningitis, reason why skull base surgeons prefer either subtemporal-transtentorial, but could not offer enough visualization of the pattern vessel for proximal control, or suboccipital-transcondylar approach, but this one requires manipulation and retraction of brainstem and cranial nerves, resulting excessive in some cases.
Other techniques have been intended to reduce blood flow in partially thrombosed giant aneurysms occluding vertebral artery in a surgical or endovascular manner, however these techniques have not demonstrated effectiveness, as some of those aneurysms keep growing, requiring surgical treatment, as reported by Cikla, who used hypothermic circulatory arrest to treat a giant vertebrobasilar junction aneurysm previously treated by coiling of the right vertebral artery with a poor result.
Endovascular treatment for large and giant partially thrombosed aneurysms includes intra-aneurysmal coiling and pattern vessel stenting, or more recently stent-alone technique, but compressive effect has not been solve for a short-term benefit.
Conclusion: Transclival approach is a direct route for clipping and decompress giant partially thrombosed vertebrobasilar junction aneurysms, as long as inherent characteristics permit it.