

RSS-Feed abonnieren
DOI: 10.1055/a-2739-2527
The adaptive traction doughnut resection technique for pyloric cancer: a case of curative resection and stenosis management
Autoren

Gastric adenocarcinoma is a leading cause of cancer-related death, but early detection allows for curative endoscopic therapies. While endoscopic submucosal dissection is the standard for early gastric cancer, its application in the pyloric ring is technically demanding due to the narrow lumen, acute angulation, and strong peristalsis, which impede stable access.
We present the case of a 71-year-old man with a 3 cm pyloric lesion confirmed as well-differentiated adenocarcinoma. To overcome the technical difficulties of this location, a “doughnut resection with adaptive traction” was performed ([Video 1]). This strategy involves a full circumferential incision around the lesion, using retroflexion in the bulb for the initial duodenal side incision followed by a circumferential incision of the gastric edge. An adaptive traction device (ATRACT, Belmont d’azergues, France) was used with one loop attached on the duodenal side and three loops on the gastric edge to facilitate exposure and increase dissection speed. Adaptive traction was done by placing the rubber band in different axes to facilitate exposure while the dissection progressed ([Fig. 1]).
This video demonstrates the “doughnut resection” technique for a circumferential pyloric adenocarcinoma, showcasing a systematic two-step dissection from both the duodenal and gastric sides to achieve a complete en-bloc resection.Video 1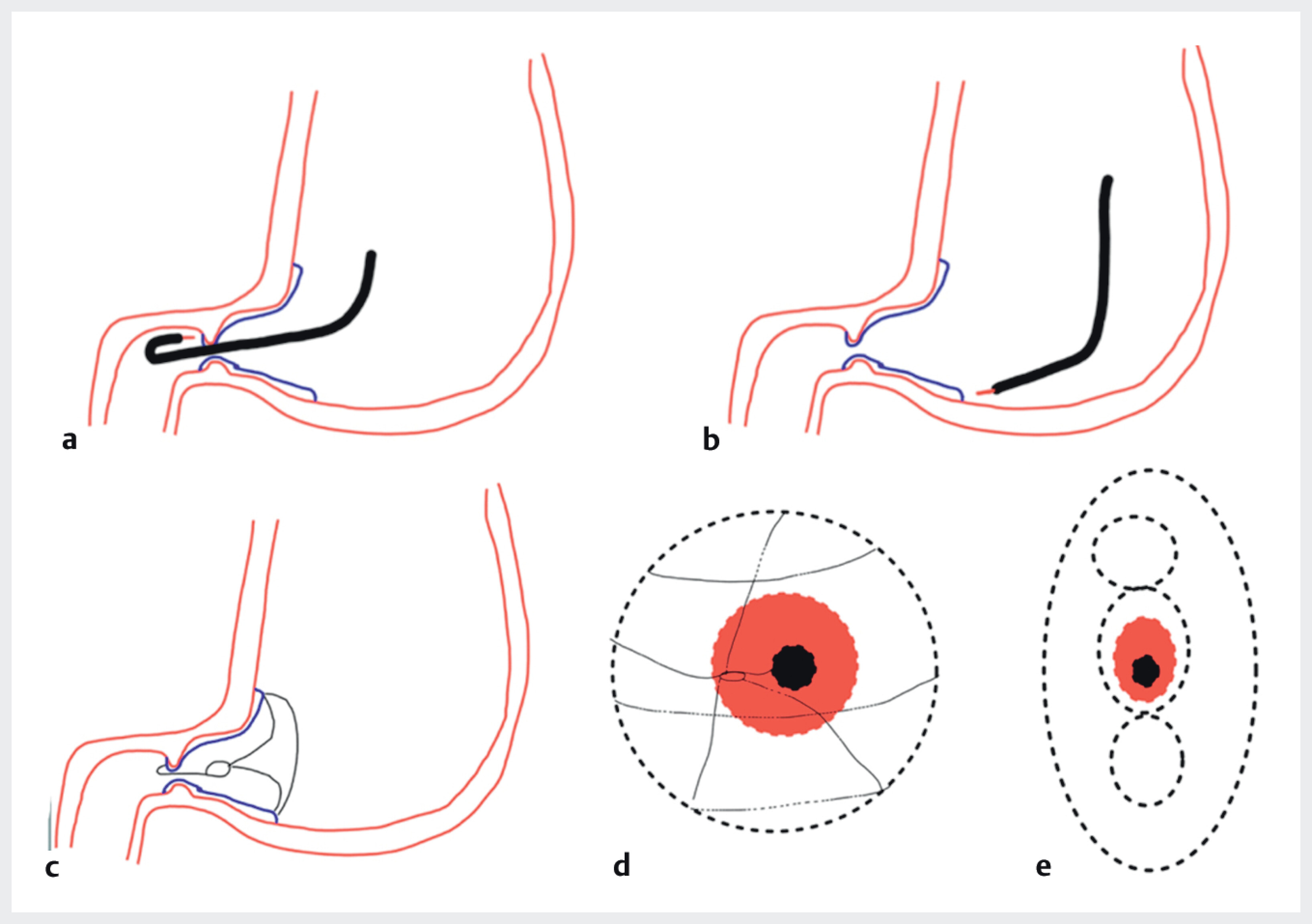
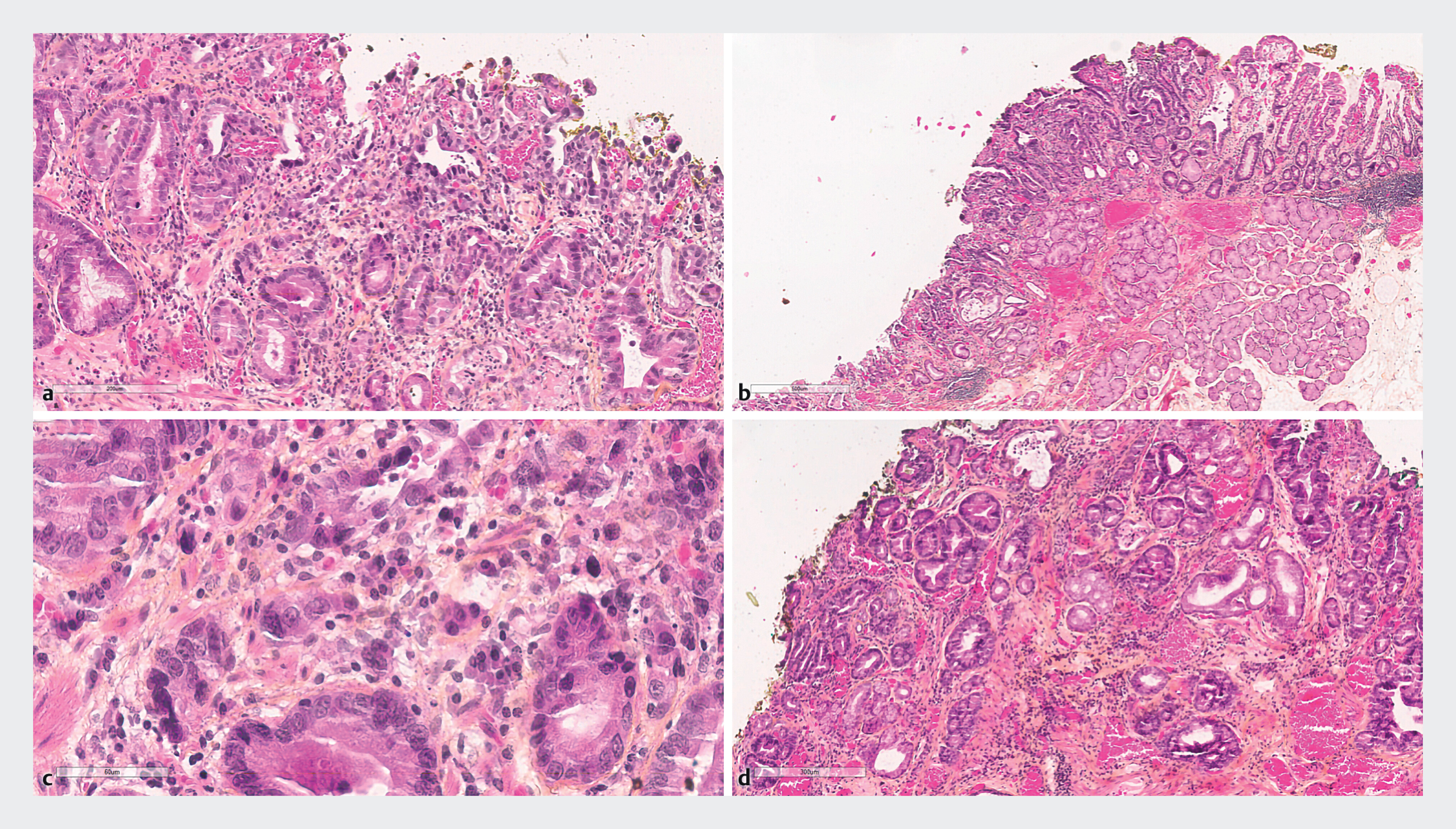
The specimen was retrieved en-bloc, and histopathology confirmed a complete R0 resection ([Fig. 2]).
One month later, the patient presented with recurrent vomiting and a 7 kg weight loss due to a tight post-operative stenosis. During endoscopy, the stricture was found to be impassable, making conventional balloon dilatation unfeasible. Consequently, a 16 mm fully covered self-expanding metal stent (Hanaro Stent) was placed, leading to the resolution of symptoms. Stent removal was planned after 1 month.
The “adaptive traction doughnut resection” technique is an effective strategy for circumferential pyloric lesions. In the cases of severe subsequent stenosis, primary stenting is a viable alternative when dilatation is not feasible.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos.
Publikationsverlauf
Artikel online veröffentlicht:
27. November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Kitamura M, Asada K, Matsuda M. et al. A novel technique of endoscopic submucosal dissection for circumferential ileocecal valve adenomas with terminal ileum involvement: the “doughnut resection” (with videos). Surg Endosc 2020; 34: 1417-1424
- 2 Yamamoto Y, Tsuji Y, Minatsuki C. et al. The pocket-creation method facilitates endoscopic submucosal dissection of gastric neoplasms involving the pyloric ring. Endoscopy 2021; 53: 1018-1023
- 3 Kim GH, Kim DH, Lee MW. et al. Factors associated with the outcomes of endoscopic submucosal dissection in pyloric neoplasms. Gastrointest Endosc 2014; 80: 618-626