

Subscribe to RSS
DOI: 10.1055/a-1236-3421
Diagnosis of biliary varices using digital cholangioscopy
Authors

A 29-year-old woman with abdominal tuberculous lymphadenitis (ATL) being treated with anti-tuberculosis drugs underwent detailed investigations for a common bile duct (CBD) stricture. Contrast-enhanced computed tomography (CECT) revealed an extrahepatic portal venous obstruction (EPVO) and a cavernous transformation of the portal vein (CTPV). The EPVO was likely caused by portal vein thrombosis due to ATL-related chronic inflammation. Testing revealed a slight elevation of serum biliary enzymes, but no jaundice. CECT suggested a CTPV-related origin for the CBD stricture ([Fig. 1a], [Fig. 1b]), which was confirmed by endoscopic ultrasound (EUS) ([Fig. 2a]); the mid to lower portion of the CBD appeared smooth on endoscopic retrograde cholangiography ([Fig. 2b]).


Intraductal ultrasonography (IDUS) showed that the narrowest point was externally compressed by multiple hypoechoic features ([Fig. 3a]). Downstream, hypoechogenic features were visible inside the CBD wall ([Fig. 3b]; arrow). These findings were suggestive of paracholedochal and epicholedochal biliary varices.

Digital cholangioscopy (Spyglass DS; Boston Scientific, Marlborough, Massachusetts, United States) showed normal mucosa in the upper CBD and confirmed compression of the CBD midportion by biliary varices. The CBD mucosa showed hyperemia with sporadic red spots and telangiectasia ([Fig. 4a], [Fig. 4b]; heads). Biliary varices were also detected in the CBD lumen, consistent with the hypoechogenic features observed on IDUS ([Fig. 5]). Interestingly, the varices were reducible by water conveyance ([Video 1]). We determined that the stricture was caused by biliary varices.

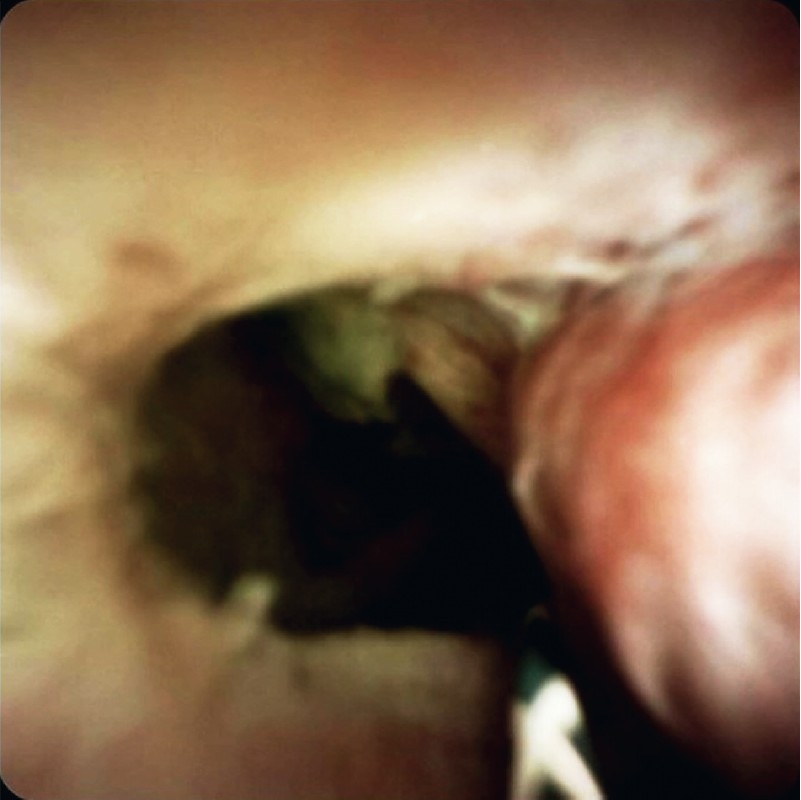
Video 1 Digital cholangioscopy of a patient with common bile duct (CBD) stricture shows a biliary varix and hyperemia of the CBD mucosa.
Despite bleeding from the biliary mucosa during biopsy, spontaneous hemostasis was achieved. We followed-up on the CBD stricture because the patient did not have obstructive jaundice.
Biliary varices are related to portal hypertension, primarily EPVO [1]. EUS [2] and IDUS [3] are useful tools for diagnosing biliary varices.
Although few reports describe cholangioscopic observations of biliary varices in detail [4] [5], we suggest that cholangioscopy is useful to diagnose biliary varices.
Publication History
Article published online:
22 September 2020
© 2020. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Dhiman RK, Behera A, Chawla YK. et al. Portal hypertensive biliopathy. Gut 2007; 56: 1001-1008
- 2 Palazzo L, Hochain P, Helmer C. et al. Biliary varices on endoscopic ultrasonography: clinical presentation and outcome. Endoscopy 2000; 32: 520-524
- 3 Takagi T, Irisawa A, Shibukawa G. et al. Intraductal ultrasonographic anatomy of biliary varices in patients with portal hypertension. Endosc Ultrasound 2015; 4: 44-51
- 4 Zulli C, Sica M, Caruso A. et al. A rare case of biliary tract stenosis caused by intraductal varices diagnosed by single-operator per-oral cholangioscopy. Gastrointest Endosc 2016; 84: 1052-1053
- 5 Phan VA, Abu-Assi R, Nguyen N. Gastrointestinal utility of per-oral cholangioscopy in the diagnosis of portal hypertension associated biliopathy. J Gastroenterol Hepatol 2016; 31: 1798